Why some jaw pain doesn’t improve with typical TMJ treatment, and what else might be going on in your body
Can a medical condition cause TMJ pain?
Yes. Conditions such as autoimmune disease, thyroid disorders, anemia, and Lyme disease can all contribute to jaw pain and TMJ symptoms, especially when standard TMJ treatment has not helped. Identifying these underlying causes is often the key to relief.
You wake up with jaw pain that feels different this time. It is in both sides of your jaw, not just one. Your jaw feels stiff in the morning, almost like your hands or knees do on a bad day. You are tired in a way that sleep does not seem to fix. And the nightguard your dentist gave you, the one that was supposed to help, has not made much of a difference.
If this sounds familiar, you are not imagining it, and you are not alone. Most jaw pain is exactly what it appears to be: a TMJ problem caused by clenching, grinding, stress, or a past injury. But for a smaller group of patients, jaw pain is one piece of a larger puzzle, one that involves the rest of the body.
You Deserve to Be Taken Seriously
If you have already tried a nightguard, physical therapy, or other standard TMJ treatments and your symptoms are not improving the way they should, that does not mean the pain is in your head. It often means there is more to the story.
At New York TMJ & Orofacial Pain, we treat TMJ disorders every day, and part of that work is recognizing when jaw pain is connected to something happening elsewhere in the body. Conditions like autoimmune disease, thyroid problems, anemia, and Lyme disease can all contribute to jaw pain, and they are often missed because no one has connected the dots between your jaw and the rest of your health.
Can a medical condition cause TMJ pain?
Yes. Conditions such as autoimmune disease, thyroid disorders, anemia, and Lyme disease can all contribute to jaw pain and TMJ symptoms, especially when standard TMJ treatment has not helped. Identifying these underlying causes is often the key to relief.
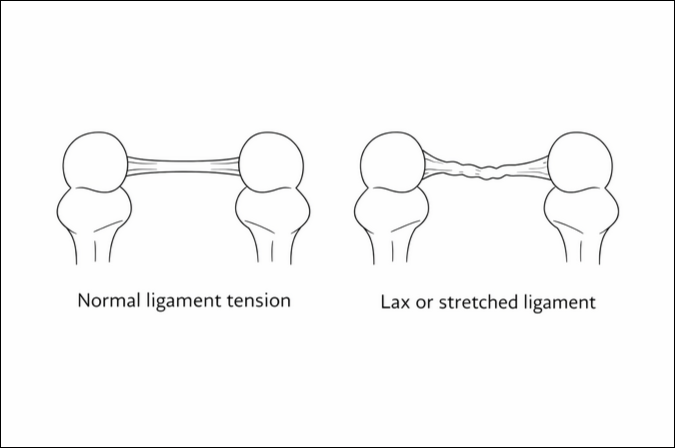
Why Your Jaw Muscles May Be the Messenger, Not the Problem
Jaw muscle pain is often a question of oxygen. Muscles that do not get enough oxygen-rich blood build up waste products that irritate nerve endings, and that irritation is what you feel as pain, aching, or fatigue in the jaw.
Two common but often overlooked issues can starve your jaw muscles of the oxygen they need.
A nervous system stuck in overdrive. Chronic stress, anxiety, or poor sleep can keep your body in a constant low-grade fight-or-flight state. One effect of that state is that blood vessels throughout the body, including in the jaw, narrow slightly and reduce blood flow to the muscles you use every day to chew, talk, and yawn.
Anemia. When your blood carries less oxygen than it should, often because of low iron, vitamin B12, or folate, your muscles fatigue and ache more easily with normal use, including the muscles of your jaw. Anemia is common and frequently goes undiagnosed until someone connects it to symptoms like this.
If your jaw pain feels disproportionate to what is actually going on in your bite or your stress level, a simple blood test checking your iron, vitamin B12, and folate levels can be a useful and inexpensive place to start.
Can Autoimmune Conditions Cause Jaw Pain?
Certain autoimmune and inflammatory conditions can directly affect the jaw joint and the muscles around it, sometimes before they are ever diagnosed.
Rheumatoid Arthritis
Rheumatoid arthritis causes inflammation in the joints, and the jaw joint is not immune. If you are noticing pain on both sides of your jaw, morning stiffness, and joint pain in your hands or wrists, it is worth mentioning this combination to your physician, since blood tests can help confirm or rule out rheumatoid involvement.
Lupus
Lupus is a condition that creates inflammation throughout the body, and that inflammation can make the entire pain system, including your jaw, more sensitive. Lupus does not always come with the well-known butterfly rash, which is part of why it can be missed. Fatigue, joint pain, and sensitivity to sunlight alongside jaw pain are worth raising with your doctor.
Psoriatic Arthritis
Psoriatic arthritis can affect the jaw joint as well, and it sometimes shows up before any skin symptoms appear. This is one reason jaw pain connected to psoriatic arthritis can be especially easy to overlook.
Hashimoto’s Thyroiditis
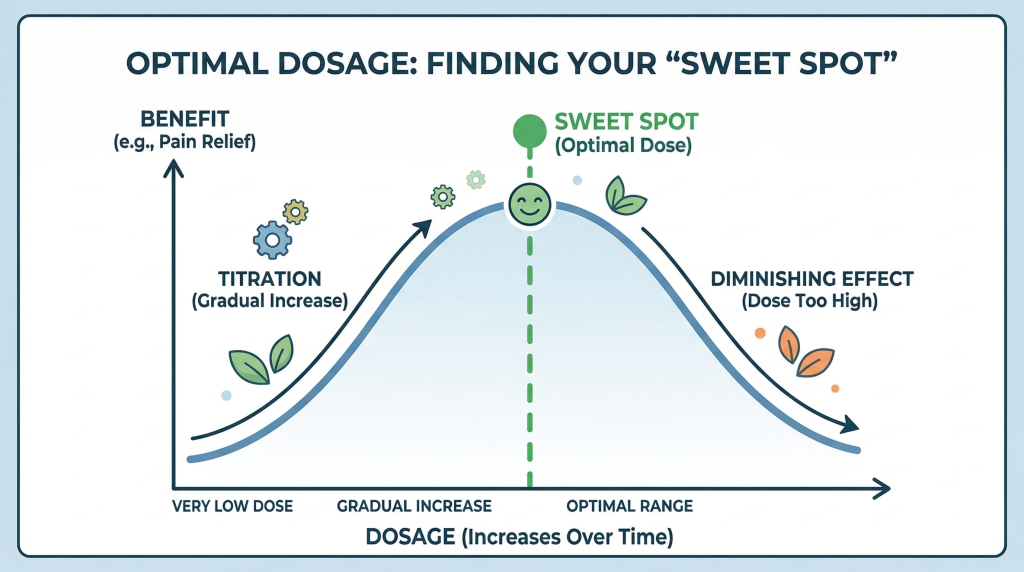
This is one of the most common conditions we see connected to jaw pain in our female patients in particular. Hashimoto’s thyroiditis slows down your thyroid, and an underactive thyroid can lead to muscle aches, joint stiffness, fatigue, and poor-quality sleep, all of which can make jaw pain worse and harder to resolve. Even thyroid levels that look technically normal on paper can still be working against you if they are not optimized for how you feel.
Can Lyme Disease Cause Jaw Pain?
If you live on Long Island, in Westchester County, or anywhere in the surrounding region, this section matters to you specifically. The northeast is the highest Lyme disease region in the country, and Lyme disease can cause joint pain, including in the jaw, sometimes without the classic bullseye rash or even a memory of a tick bite.
If you are dealing with jaw pain alongside fatigue or pain in other joints, and you spend time outdoors in our area, it is worth asking your doctor about Lyme testing, even if nothing about a tick bite comes to mind.
You Are Not Starting From Scratch
Finding out that something beyond your jaw may be contributing to your pain is not bad news. It is often the missing piece that finally makes your symptoms make sense, and the first real step toward a plan that actually works for you.
Orofacial pain specialists take the time to look at the whole picture, not just your jaw in isolation. When they suspect something systemic may be involved, they will collaborate closely with your physician, rheumatologist, or other specialists so that your care is coordinated rather than fragmented.
Are You Experiencing Jaw Pain That Isn't Responding to Treatment in the NYC Metropolitan Area?
If you’re in the New York City metropolitan area and you’ve been dealing with jaw pain that hasn’t improved with standard treatment, you deserve answers, not just temporary relief.
At New York TMJ & Orofacial Pain, we specialize exclusively in diagnosing and treating TMJ disorders and orofacial pain. We take time to identify the true cause of your symptoms and build a treatment plan that directly addresses it, including coordinating with your physician when a medical condition may be contributing to your pain.
We have 4 locations: Midtown Manhattan, White Plains, Hauppauge, and Springfield, NJ.
Contact us today to schedule a comprehensive evaluation. →About the Author
Dr. Donald R. Tanenbaum is a board-certified specialist who has dedicated his 40-year career to diagnosing and treating Orofacial Pain, TMD/TMJ, headache, and sleep-related breathing disorders. He practices in our Manhattan and Hauppauge offices.
What to Expect at Your First Visit →
Frequently Asked Questions About Medical Conditions That Can Cause TMJ Pain
Can autoimmune diseases cause TMJ pain?
Yes. Conditions such as rheumatoid arthritis, lupus, psoriatic arthritis, and Hashimoto’s thyroiditis can all contribute to jaw pain, jaw joint inflammation, and muscle dysfunction. In some cases, jaw symptoms appear before the underlying condition is even diagnosed.
Can anemia cause jaw muscle pain?
Yes. Anemia reduces the amount of oxygen your blood can deliver to muscles, including your jaw muscles, which can lead to fatigue, cramping, and aching with normal use like chewing or talking.
Can Lyme disease affect the jaw joint?
Yes. Lyme disease can cause joint pain, including in the jaw joint, and this is a particular concern for patients in Long Island, Westchester County, and other parts of the northeastern United States where Lyme disease is common.
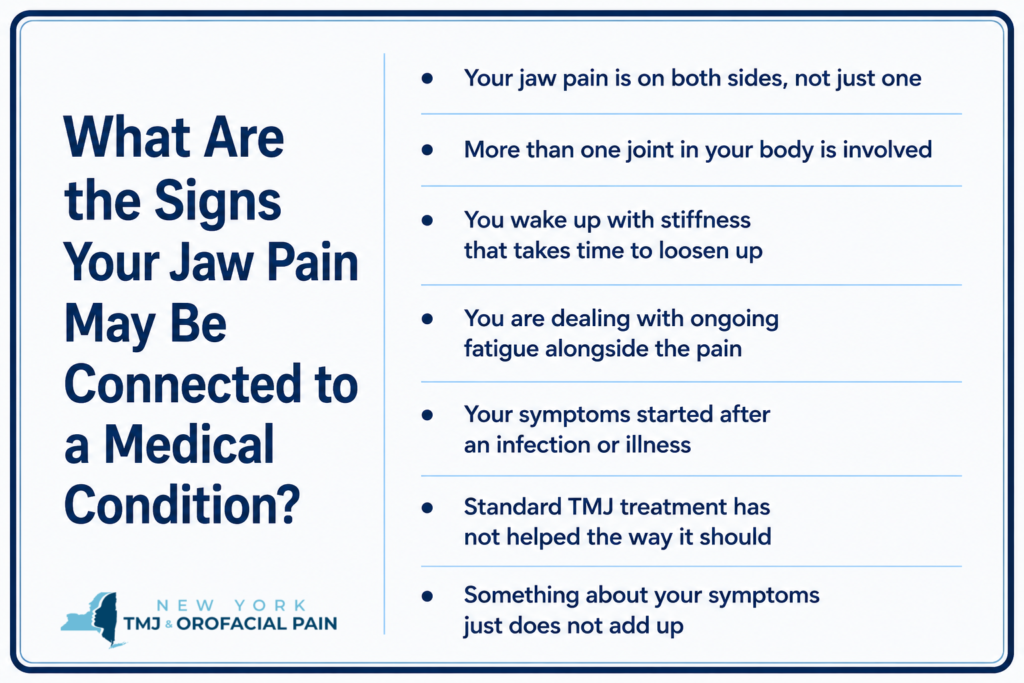
How do I know if my jaw pain is connected to a medical condition?
Some signs to watch for include pain on both sides of the jaw, involvement of other joints, morning stiffness, ongoing fatigue, symptoms that began after an illness, or jaw pain that has not responded to standard TMJ treatment. If any of these sound familiar, it is worth discussing a broader medical evaluation with your provider.
What should I do if I think something more than TMJ is going on?
Start by talking with your dentist, physician, or an orofacial pain specialist. A thorough evaluation, sometimes including blood work, can help determine whether a medical condition is contributing to your jaw pain and guide you toward the right treatment plan.