When the issue is joint instability, not tightness
If your jaw opens very wide, clicks frequently, and feels loose or fatigued, TMJ hypermobility may be the underlying cause. This type of TMJ disorder is driven by joint instability, not restriction, and requires a specialized approach to treatment.
When Your Symptoms Do Not Fit the Usual Pattern
Most people assume TMJ problems come from a jaw that is tight or stuck.
But some patients experience the opposite.
Your jaw may open very wide. You may hear clicking or feel shifting in the joint. Instead of restriction, it can feel loose or unreliable. The muscles around it often feel constantly tired or sore, even when you are not doing much.
If this sounds familiar, TMJ hypermobility may be part of the picture. The issue is not too little movement. It is too much. In our practice in the New York City metropolitan area, we see this pattern more often than many patients expect.
The Role of TMJ Hypermobility – Why the Jaw Becomes Painful
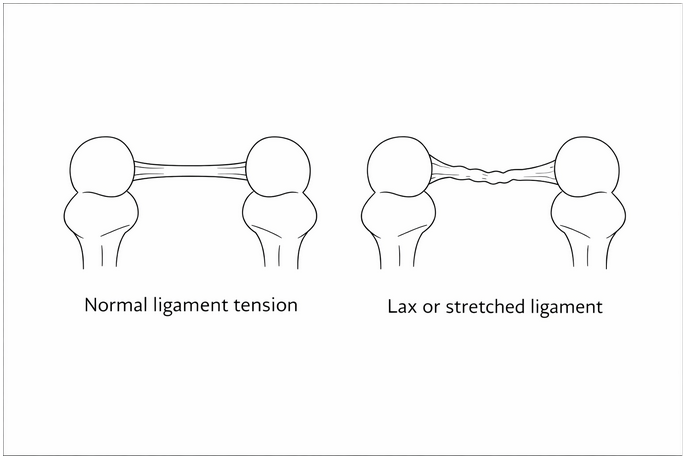
Hypermobility means your joints move beyond the normal range.
For some people, that simply means they are flexible. For others, it reflects a connective tissue condition such as Ehlers-Danlos Syndrome.
These conditions affect collagen, the material that gives structure and support to ligaments and joints. When collagen is more elastic than it should be, the joint is not held as firmly. It moves more than it should, and the body has to compensate.
In TMJ hypermobility, that compensation falls on the muscles.
Why the Jaw Becomes Painful
When the joint lacks stability, the muscles step in to control it.
At first, this works. Over time, it becomes a problem.
The muscles are constantly active, trying to keep the joint steady. This leads to fatigue, soreness, and persistent discomfort. Many patients also notice clicking or popping, which often reflects instability inside the joint rather than something harmless.
This is what makes TMJ hypermobility different.
Instead of a jaw that cannot open enough, this is a joint that moves too much and lacks control.
A Common Pattern
In our practice, we often see patients who have always been “flexible.”
They may have a history of joint issues in other parts of the body. Ankles that sprain easily. Shoulders that feel unstable. Pain that takes longer than expected to resolve.
Some already have a diagnosis of hypermobility or Ehlers-Danlos Syndrome. Others have never connected these patterns before.
When the connection is made, their jaw symptoms finally start to make sense.
Why Treatment Has Not Worked
Many patients with TMJ hypermobility have already tried treatment.
They are often told to relax their muscles or adjust their bite. Sometimes this helps temporarily, but the symptoms return.
That is because the underlying issue is instability.
In a hypermobile joint, small strains do not fully resolve. The joint remains less supported, and the muscles continue to compensate. Over time, they become overworked and sensitive.
This does not mean improvement is not possible. It means the approach needs to change.
Treatment Focus: Stability and Control
The goal is not to change the underlying connective tissue.
The goal is to improve stability and reduce strain on the system.
This often involves reducing clenching and jaw tension during the day and protecting the joint at night with an oral appliance. Patients are also guided to avoid extreme opening, such as wide yawning or large bites.
Physical therapy plays an important role, but the focus is different. Instead of just relaxing muscles, the emphasis is on controlled strengthening and stabilization.
When muscle pain is persistent, targeted treatments may be used to help calm the system.
In some cases, therapies that support ligament strength may also be considered.
Setting the Right Expectations
With hypermobility or Ehlers-Danlos Syndrome, the underlying tissue does not change.
But that does not mean nothing can improve.
When treatment focuses on stability, protection, and control, patients often experience less pain, better function, and more confidence in how their jaw feels.
When to Seek Evaluation
If your jaw opens unusually wide, clicks along with pain or fatigue, or has not improved with previous care, it may be worth a more specialized evaluation.
This is especially true if you have been diagnosed with hypermobility or Ehlers-Danlos Syndrome, or suspect that you may be more flexible than average.
Moving Forward
If your symptoms have never quite fit the typical TMJ pattern, there is usually a reason.
Recognizing that TMJ hypermobility is often the turning point in getting the right diagnosis and treatment.
TMJ disorders affect women far more often than men.
This is not a coincidence. Differences in joint structure, hormones, and pain processing can make symptoms more likely to develop and harder to resolve.
Understanding why is often the first step toward real, lasting relief.
If you’re a woman dealing with TMJ symptoms such as jaw pain, clicking, locking, tightness, frequent headaches, or facial pain, this is for you.
I’m a board-certified orofacial pain specialist and have been treating people with TMJ symptoms for over 40 years. The majority of patients who come to our NYC practice are women. In fact, close to 70% of people seeking treatment for TMJ disorders are women.
There are biological reasons for this huge disparity, and understanding them can be essential if you are struggling to feel better.
Helping Patients Better Understand Their Persistent Symptoms
Many women come to us looking for a reason why their jaw continues to hurt, though they have used a nightguard, taken anti – inflammatory medications, and followed a soft diet for months.
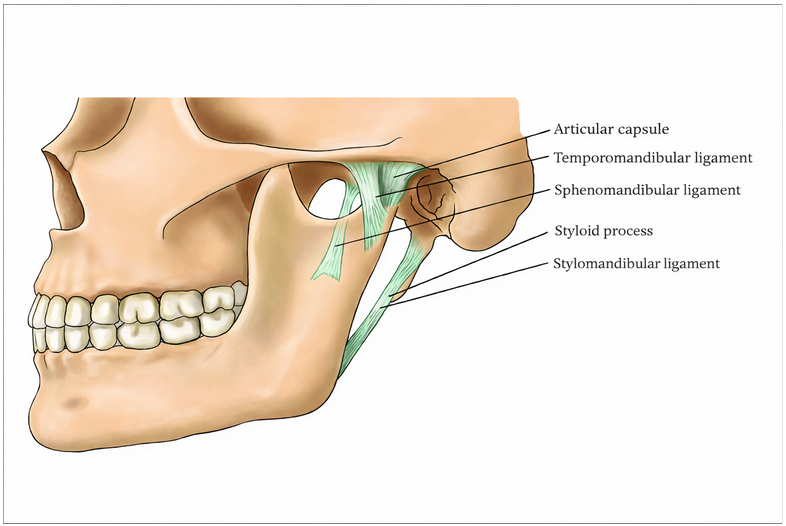
TMJ (the clinical term is temporomandibular joint disorder, or TMD) involves the interaction between your joints, your muscles, and your nervous system. According to the National Institute of Dental and Craniofacial Research, these disorders are among the most common causes of facial pain.
TMJ symptoms are not something you’re imagining. They are what your body is expressing.
Why This Happens in Women
1. The ligaments in your temporomandibular joint are more flexible and less stable
In women, the ligaments in the temporomandibular joint tend to be more flexible and less structurally stable than in men.
There is a reason for this! The temporomandibular joint in women contains an abundance of estrogen receptors, making its tissues directly responsive to hormonal fluctuation. In fact, estrogen promotes elastin production, producing ligaments that are more flexible and less structurally organized than those in men. The result is greater joint laxity and reduced load-bearing capacity. In women, this means that the temporomandibular joint is more susceptible to compromise with everyday function, and certainly when under excessive loading during daytime jaw overuse behaviors and sleep grinding and clenching of the teeth.
More stable joint ligaments tolerate these stresses longer. More flexible ligaments reach their limits sooner.
That is why symptoms can emerge more commonly in the temporomandibular joints in women over time.
2. The female brain processes pain differently
Pain is not just about what is happening in a body part. It is also about how your brain processes pain signals.
Men generally have stronger central nervous system modulating elements for dampening pain signals. Women, on average, have less of that built-in inhibition due to the lack of Androgens, including testosterone and related hormones. In practical terms, male hormones strengthen the brain’s capacity to send dampening signals down to pain receptors throughout the body. Women, carrying lower androgen levels, lack this same degree of biological protection
This means that the same level of inflammation and tissue injury generated pain can be experienced very differently.
What might feel like temporary soreness in a man can become persistent pain in a woman.
This is not about tolerance or resilience. It reflects real biological differences in how the nervous system regulates pain.
3. Stress has a greater physical impact on a woman’s jaw
Stress affects everyone, but it often shows up differently in women than it does in men, again for biological reasons.
Under prolonged stress, the human body can remain in an activated state, often with accompanying muscle tension. This is called sympathetic activation. Over time, this activation can deplete the neurotransmitters that support descending pain modulation, the very system that blunts pain experiences on a daily basis. With research suggesting that women have less robust pain blunting systems than men, the pain that results from ongoing muscle tension can be more profound in women and recovery even in the presence of care taking longer.
In the jaw specifically, muscle pain and fatigue as a result of stress-driven daytime clenching and night grinding can be impactful and persistent
Men can experience this as well, but women tend to develop more sustained symptoms, which increases the overall load on the system.
The Emergence of TMJ Symptoms
In our NYC metropolitan area practices, we commonly see TMJ symptoms develop as a result of a specific traumatic event, a mind-body disorder that drives persistent muscle tension, or an underlying medical condition that reduces tissue resiliency in the jaw muscles and temporomandibular joints.
Sometimes multiple factors are responsible, and symptoms develop gradually.
First, the body adapts. Then it begins to struggle. In women, as a result of the biological factors mentioned, the likelihood of a TMJ problem emerging and hanging around increases. At times, TMJ symptoms such as jaw pain, clicking, locking, tightness, frequent headaches, or facial pain no longer resolve on their own but require explanation and formal treatment.
A More Complete Understanding for Women
Biological vulnerability is real, but it does not mean that tissue healing and feeling better are not achievable. With the right evaluation, the causes and risk factors can be addressed comprehensively with education and a wide variety of supportive treatments that lead to meaningful and sustainable improvement.
Are You a Woman Experiencing TMJ Symptoms in the NYC Metropolitan Area?
If you are dealing with persistent jaw pain, clicking, locking, tightness, frequent headaches, or facial pain, there is a reason why.
At New York TMJ & Orofacial Pain, we specialize in diagnosing and treating TMJ disorders and orofacial pain. We take the time to understand what is actually driving your symptoms and build a treatment plan around it.
Our team of orofacial pain specialists provides evidence-based, individualized care at our locations in the NYC metropolitan area. We work closely with each patient and often other healthcare providers to restore comfort and function.
If your symptoms have persisted despite reassurance or prior treatment, a more specialized evaluation can make all the difference.
The Jaw Surgery Worked – But the Pain Didn’t Go Away
What low-dose naltrexone can do for persistent neuropathic facial pain
Your jaw surgery went well. The imaging looks fine. Your surgeon says everything healed the way it should.
And yet, you have pain. It aches along your jaw. The sensation feels, as one of our patients put it, like “my skin is sunburnt” – even though nothing is visibly wrong.
If this sounds familiar, you are not imagining it. And you are not alone.
Persistent pain after facial or jaw surgery is a recognized clinical reality. It has a name, a mechanism, and – importantly – treatment options that go beyond what most patients are ever offered.
Your Pain Is Real. And It Has a Medical Explanation.
One of the most disorienting experiences our patients describe is being told that everything looks fine, yet they still live with daily pain.
When surgery corrects a structural problem, but pain continues, the issue often isn’t structural at all. It’s neurological. The nervous system, particularly the pain-signaling pathways, can remain in an activated state long after the original source of injury has been addressed.
This is called neuropathic pain – pain that originates in your nervous system itself, not in damaged tissue. In some cases, it takes on a more complex form called nociplastic pain, a term from the International Association for the Study of Pain that describes pain arising from altered signaling in the central nervous system, without ongoing tissue damage to account for it.
In plain terms: your brain’s pain system has become hypersensitive. It keeps sending pain signals even after the original problem has been treated. This is not a character flaw, a low pain threshold, or something you should simply push through. It is a measurable, treatable condition.
A Case We Treated: Debbie’s Story
“Debbie” was a 52-year-old woman from the New York City area who came to us with a problem that had no easy answer.
Two years earlier, she had undergone bilateral TMJ total joint replacement – a significant surgery to address severe, progressive jaw degeneration. The procedure went well. Her jaw opened better. Imaging confirmed the prosthetics were stable. By every measurable standard, surgery was a success.
But Debbie was in constant pain.
She described a burning sensation along both sides of her jaw and temples. It was relentless, unpleasant, and unlike anything she had experienced before the surgery. She had tried NSAIDs, benzodiazepines, opioids, and anticonvulsant medications. None helped. Several caused side effects severe enough to stop.
When she arrived at our practice, the examination revealed something important: light touch to the affected areas caused heightened sensitivity and a kind of distorted sensation. This told us that her issue wasn’t structural, but neurological. Her pain wasn’t coming from the joint. It was coming from a sensitized nervous system.
This is where a mechanism-based approach – asking not just what is causing pain, but how and why her pain system had become dysregulated – becomes essential.
Introducing Low-Dose Naltrexone (LDN)
Low-dose naltrexone is used off-label for neuropathic and centrally mediated facial pain conditions.
What Is Low-Dose Naltrexone (LDN?)
Naltrexone is a medication with a long track record in addiction medicine, typically prescribed at 50 to 100 mg daily. Low-dose naltrexone (LDN) refers to the same medication prescribed at a fraction of that dose – generally 1.5 to 6 mg daily – where it appears to work through an entirely different set of mechanisms. LDN is obtained through a compounding pharmacy and used off-label for centrally mediated and neuropathic pain conditions.
Naltrexone is a medication with a long track record in addiction medicine when used in large doses. But at a fraction of that dose, it appears to work through an entirely different set of mechanisms, ones that are particularly relevant to persistent, centrally mediated pain.
This low-dose application is called Low-Dose Naltrexone (LDN).
How Low-Dose Naltrexone Works: Two Mechanisms That Matter
1. Low-Dose Naltrexone helps your body produce more of its own natural pain-relievers.
At low doses, naltrexone temporarily and mildly blocks the body’s opioid receptors for a few hours. The body responds by producing more endorphins, which are its own natural pain-modulating molecules. When the mild blockade resolves, those elevated endorphins flood back into the system. The result is a net increase in the body’s own pain-relief capacity.
2. It calms an overactivated immune response in the brain.
The central nervous system contains immune cells called microglia. In patients with chronic or neuropathic pain, microglia can become chronically activated, releasing inflammatory signals that amplify pain. LDN appears to reduce this microglial activation, quieting the neuroinflammatory response that keeps pain pathways in a heightened state.
Together, these two mechanisms address something many conventional pain medications do not: the underlying nervous system dysregulation driving persistent pain.
How Low-Dose Naltrexone Is Prescribed
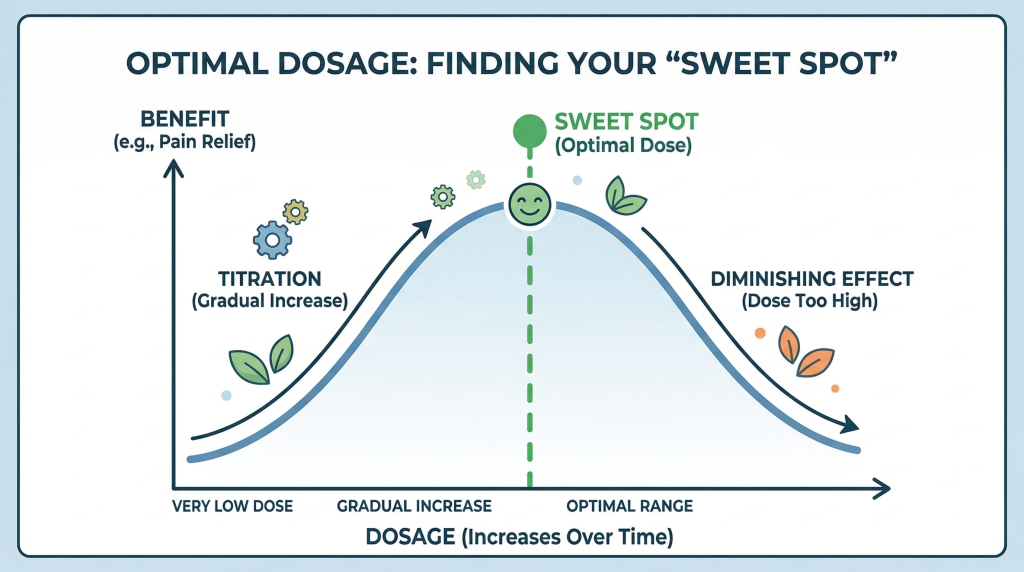
Treatment typically begins at a very low dose nightly, with gradual increases every two to three weeks, depending on how you respond.
One of the most important things to understand about LDN is that more is not necessarily better. There is what clinicians describe as a “sweet spot”, an optimal dose where the benefit peaks. Going above that range can actually diminish the effect. This is why individualized, carefully supervised titration matters.
LDN is generally well tolerated. The most commonly reported side effects are vivid dreams, mild insomnia, or light nausea, but they are usually transient and dose-dependent. Importantly, LDN cannot be used concurrently with opioid medications, as it would block their effect.
What Happened with Debbie
Debbie began LDN nightly. After minimal change, we increased the dose and within days, her burning pain had begun to decrease substantially.
At her two-month follow-up, she described the change this way: she could still feel her face, but the sensation was no longer unpleasant or painful. After years of burning, that distinction was everything.
“She could still feel her face – but the sensation was no longer unpleasant or painful.”
Common Misconceptions About Post-Surgical Pain
Patients with persistent pain after facial or jaw surgery often encounter frustrating responses from providers who haven’t yet connected the dots between mechanism and treatment. Here is what we often hear and what the evidence actually says:
“If the surgery worked, you should be pain-free.”
Structural success does not always equal pain resolution. Neuropathic and nociplastic pain can persist independently of tissue healing.
“There is nothing left to try.”
Mechanism-based options like LDN are often not explored until later in a patient’s journey – if at all. They represent a distinct category from conventional neuropathic medications.
“It may be psychological.”
Nociplastic pain involves measurable central nervous system changes. It is not “in your head” – though behavioral and psychological factors can influence how any pain is experienced, as they do with all chronic conditions.
Who May Benefit from This Approach
Low-dose naltrexone may be an appropriate consideration for you if you experience:
Persistent burning or aching pain following TMJ surgery
Post-surgical facial pain with negative or stable imaging
Neuropathic facial pain that has not responded to standard medications
Persistent idiopathic facial pain
Burning mouth syndrome
Chronic headache or orofacial pain with a centrally mediated component
Patient selection and dose titration are essential. This is not a first-line treatment for acute or clearly structural pain. Instead, it is a targeted option for a specific mechanism.
Our Approach: Finding the “Why” Before the “What”
At New York TMJ & Orofacial Pain, we do not begin with a treatment. We begin with a question: what is actually driving your pain?
For patients like Debbie, that question led to an answer that changed everything. Her pain was not structural. It was neurological. And once we understood the mechanism, we could target it directly.
That same principle applies across the full range of conditions we treat. Whether the pain stems from muscle dysfunction, joint pathology, nerve sensitization, or a combination of factors, our goal is always the same: identify the true cause and build a plan around it, not around generic protocols.
LDN is one tool within that framework. It is not right for every patient. But for the right patient, it can offer relief that nothing else has.
Are You Experiencing Persistent Facial Pain in the NYC Metropolitan Area?
If you have had facial or jaw surgery, or if you’ve been living with facial pain that no one has been able to explain, you deserve more than temporary relief. You deserve answers.
At New York TMJ & Orofacial Pain, we specialize exclusively in diagnosing and treating TMJ disorders and orofacial pain. We take the time to identify the true cause of your symptoms and build a treatment plan that directly addresses it.
We have four convenient locations across the region, staffed with experienced orofacial pain specialists:
Midtown Manhattan
White Plains
Hauppauge, Long Island
Springfield, New Jersey
Contact us today to schedule a comprehensive evaluation.
Dr. John Dinan is a board-certified Orofacial Pain specialist dedicated to the treatment of TMJ/TMD disorders and related conditions. He practices in our Manhattan and Springfield, NJ offices.