The Jaw Surgery Worked – But the Pain Didn’t Go Away
What low-dose naltrexone can do for persistent neuropathic facial pain
Your jaw surgery went well. The imaging looks fine. Your surgeon says everything healed the way it should.
And yet, you have pain. It aches along your jaw. The sensation feels, as one of our patients put it, like “my skin is sunburnt” – even though nothing is visibly wrong.
If this sounds familiar, you are not imagining it. And you are not alone.
Persistent pain after facial or jaw surgery is a recognized clinical reality. It has a name, a mechanism, and – importantly – treatment options that go beyond what most patients are ever offered.
Your Pain Is Real. And It Has a Medical Explanation.
One of the most disorienting experiences our patients describe is being told that everything looks fine, yet they still live with daily pain.
When surgery corrects a structural problem, but pain continues, the issue often isn’t structural at all. It’s neurological. The nervous system, particularly the pain-signaling pathways, can remain in an activated state long after the original source of injury has been addressed.
This is called neuropathic pain – pain that originates in your nervous system itself, not in damaged tissue. In some cases, it takes on a more complex form called nociplastic pain, a term from the International Association for the Study of Pain that describes pain arising from altered signaling in the central nervous system, without ongoing tissue damage to account for it.
In plain terms: your brain’s pain system has become hypersensitive. It keeps sending pain signals even after the original problem has been treated. This is not a character flaw, a low pain threshold, or something you should simply push through. It is a measurable, treatable condition.
A Case We Treated: Debbie’s Story
“Debbie” was a 52-year-old woman from the New York City area who came to us with a problem that had no easy answer.
Two years earlier, she had undergone bilateral TMJ total joint replacement – a significant surgery to address severe, progressive jaw degeneration. The procedure went well. Her jaw opened better. Imaging confirmed the prosthetics were stable. By every measurable standard, surgery was a success.
But Debbie was in constant pain.
She described a burning sensation along both sides of her jaw and temples. It was relentless, unpleasant, and unlike anything she had experienced before the surgery. She had tried NSAIDs, benzodiazepines, opioids, and anticonvulsant medications. None helped. Several caused side effects severe enough to stop.
When she arrived at our practice, the examination revealed something important: light touch to the affected areas caused heightened sensitivity and a kind of distorted sensation. This told us that her issue wasn’t structural, but neurological. Her pain wasn’t coming from the joint. It was coming from a sensitized nervous system.
This is where a mechanism-based approach – asking not just what is causing pain, but how and why her pain system had become dysregulated – becomes essential.
Introducing Low-Dose Naltrexone (LDN)

What Is Low-Dose Naltrexone (LDN?)
Naltrexone is a medication with a long track record in addiction medicine, typically prescribed at 50 to 100 mg daily. Low-dose naltrexone (LDN) refers to the same medication prescribed at a fraction of that dose – generally 1.5 to 6 mg daily – where it appears to work through an entirely different set of mechanisms. LDN is obtained through a compounding pharmacy and used off-label for centrally mediated and neuropathic pain conditions.
Naltrexone is a medication with a long track record in addiction medicine when used in large doses. But at a fraction of that dose, it appears to work through an entirely different set of mechanisms, ones that are particularly relevant to persistent, centrally mediated pain.
This low-dose application is called Low-Dose Naltrexone (LDN).
How Low-Dose Naltrexone Works: Two Mechanisms That Matter
1. Low-Dose Naltrexone helps your body produce more of its own natural pain-relievers.
At low doses, naltrexone temporarily and mildly blocks the body’s opioid receptors for a few hours. The body responds by producing more endorphins, which are its own natural pain-modulating molecules. When the mild blockade resolves, those elevated endorphins flood back into the system. The result is a net increase in the body’s own pain-relief capacity.
2. It calms an overactivated immune response in the brain.
The central nervous system contains immune cells called microglia. In patients with chronic or neuropathic pain, microglia can become chronically activated, releasing inflammatory signals that amplify pain. LDN appears to reduce this microglial activation, quieting the neuroinflammatory response that keeps pain pathways in a heightened state.
Together, these two mechanisms address something many conventional pain medications do not: the underlying nervous system dysregulation driving persistent pain.
How Low-Dose Naltrexone Is Prescribed
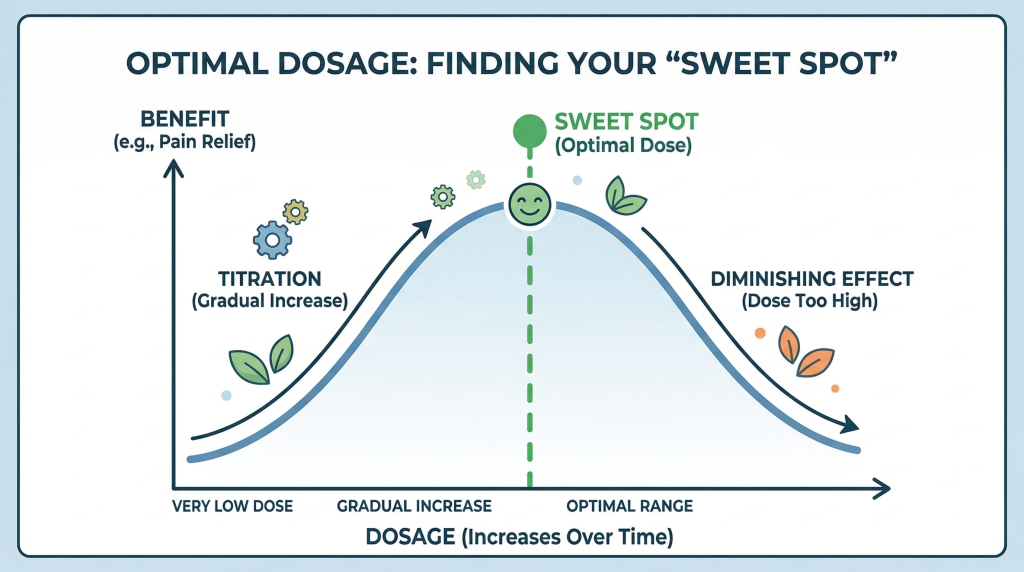
Treatment typically begins at a very low dose nightly, with gradual increases every two to three weeks, depending on how you respond.
One of the most important things to understand about LDN is that more is not necessarily better. There is what clinicians describe as a “sweet spot”, an optimal dose where the benefit peaks. Going above that range can actually diminish the effect. This is why individualized, carefully supervised titration matters.
LDN is generally well tolerated. The most commonly reported side effects are vivid dreams, mild insomnia, or light nausea, but they are usually transient and dose-dependent. Importantly, LDN cannot be used concurrently with opioid medications, as it would block their effect.
What Happened with Debbie
Debbie began LDN nightly. After minimal change, we increased the dose and within days, her burning pain had begun to decrease substantially.
At her two-month follow-up, she described the change this way: she could still feel her face, but the sensation was no longer unpleasant or painful. After years of burning, that distinction was everything.
“She could still feel her face – but the sensation was no longer unpleasant or painful.”
Common Misconceptions About Post-Surgical Pain
Patients with persistent pain after facial or jaw surgery often encounter frustrating responses from providers who haven’t yet connected the dots between mechanism and treatment. Here is what we often hear and what the evidence actually says:
“If the surgery worked, you should be pain-free.”
Structural success does not always equal pain resolution. Neuropathic and nociplastic pain can persist independently of tissue healing.
“There is nothing left to try.”
Mechanism-based options like LDN are often not explored until later in a patient’s journey – if at all. They represent a distinct category from conventional neuropathic medications.
“It may be psychological.”
Nociplastic pain involves measurable central nervous system changes. It is not “in your head” – though behavioral and psychological factors can influence how any pain is experienced, as they do with all chronic conditions.
Who May Benefit from This Approach
Low-dose naltrexone may be an appropriate consideration for you if you experience:
- Persistent burning or aching pain following TMJ surgery
- Post-surgical facial pain with negative or stable imaging
- Neuropathic facial pain that has not responded to standard medications
- Persistent idiopathic facial pain
- Burning mouth syndrome
- Chronic headache or orofacial pain with a centrally mediated component
Patient selection and dose titration are essential. This is not a first-line treatment for acute or clearly structural pain. Instead, it is a targeted option for a specific mechanism.
Our Approach: Finding the “Why” Before the “What”
At New York TMJ & Orofacial Pain, we do not begin with a treatment. We begin with a question: what is actually driving your pain?
For patients like Debbie, that question led to an answer that changed everything. Her pain was not structural. It was neurological. And once we understood the mechanism, we could target it directly.
That same principle applies across the full range of conditions we treat. Whether the pain stems from muscle dysfunction, joint pathology, nerve sensitization, or a combination of factors, our goal is always the same: identify the true cause and build a plan around it, not around generic protocols.
LDN is one tool within that framework. It is not right for every patient. But for the right patient, it can offer relief that nothing else has.
Are You Experiencing Persistent Facial Pain in the NYC Metropolitan Area?
If you have had facial or jaw surgery, or if you’ve been living with facial pain that no one has been able to explain, you deserve more than temporary relief. You deserve answers.
At New York TMJ & Orofacial Pain, we specialize exclusively in diagnosing and treating TMJ disorders and orofacial pain. We take the time to identify the true cause of your symptoms and build a treatment plan that directly addresses it.
We have four convenient locations across the region, staffed with experienced orofacial pain specialists:
- Midtown Manhattan
- White Plains
- Hauppauge, Long Island
- Springfield, New Jersey
Contact us today to schedule a comprehensive evaluation.
https://www.nytmj.com/contact-us-locations/
About the Author
Dr. John Dinan is a board-certified Orofacial Pain specialist dedicated to the treatment of TMJ/TMD disorders and related conditions. He practices in our Manhattan and Springfield, NJ offices.
Read: Trigeminal Neuralgia and the Experience of Tooth Pain →