TMJ disorders affect women far more often than men.
This is not a coincidence. Differences in joint structure, hormones, and pain processing can make symptoms more likely to develop and harder to resolve.
Understanding why is often the first step toward real, lasting relief.
If you’re a woman dealing with TMJ symptoms such as jaw pain, clicking, locking, tightness, frequent headaches, or facial pain, this is for you.
I’m a board-certified orofacial pain specialist and have been treating people with TMJ symptoms for over 40 years. The majority of patients who come to our NYC practice are women. In fact, close to 70% of people seeking treatment for TMJ disorders are women.
There are biological reasons for this huge disparity, and understanding them can be essential if you are struggling to feel better.
Helping Patients Better Understand Their Persistent Symptoms
Many women come to us looking for a reason why their jaw continues to hurt, though they have used a nightguard, taken anti – inflammatory medications, and followed a soft diet for months.
TMJ (the clinical term is temporomandibular joint disorder, or TMD) involves the interaction between your joints, your muscles, and your nervous system. According to the National Institute of Dental and Craniofacial Research, these disorders are among the most common causes of facial pain.
TMJ symptoms are not something you’re imagining. They are what your body is expressing.
Why This Happens in Women
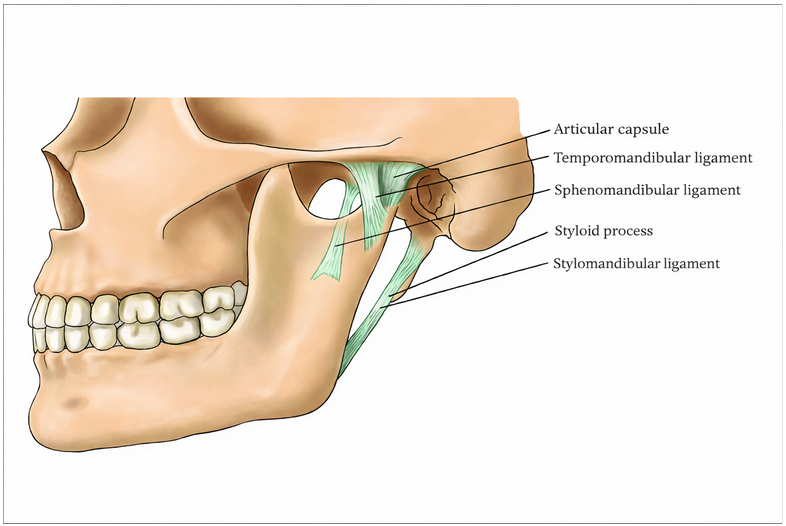
1. The ligaments in your temporomandibular joint are more flexible and less stable
In women, the ligaments in the temporomandibular joint tend to be more flexible and less structurally stable than in men.
There is a reason for this! The temporomandibular joint in women contains an abundance of estrogen receptors, making its tissues directly responsive to hormonal fluctuation. In fact, estrogen promotes elastin production, producing ligaments that are more flexible and less structurally organized than those in men. The result is greater joint laxity and reduced load-bearing capacity. In women, this means that the temporomandibular joint is more susceptible to compromise with everyday function, and certainly when under excessive loading during daytime jaw overuse behaviors and sleep grinding and clenching of the teeth.
More stable joint ligaments tolerate these stresses longer. More flexible ligaments reach their limits sooner.
That is why symptoms can emerge more commonly in the temporomandibular joints in women over time.
2. The female brain processes pain differently
Pain is not just about what is happening in a body part. It is also about how your brain processes pain signals.
Men generally have stronger central nervous system modulating elements for dampening pain signals. Women, on average, have less of that built-in inhibition due to the lack of Androgens, including testosterone and related hormones. In practical terms, male hormones strengthen the brain’s capacity to send dampening signals down to pain receptors throughout the body. Women, carrying lower androgen levels, lack this same degree of biological protection
This means that the same level of inflammation and tissue injury generated pain can be experienced very differently.
What might feel like temporary soreness in a man can become persistent pain in a woman.
This is not about tolerance or resilience. It reflects real biological differences in how the nervous system regulates pain.
3. Stress has a greater physical impact on a woman’s jaw

Stress affects everyone, but it often shows up differently in women than it does in men, again for biological reasons.
Under prolonged stress, the human body can remain in an activated state, often with accompanying muscle tension. This is called sympathetic activation. Over time, this activation can deplete the neurotransmitters that support descending pain modulation, the very system that blunts pain experiences on a daily basis. With research suggesting that women have less robust pain blunting systems than men, the pain that results from ongoing muscle tension can be more profound in women and recovery even in the presence of care taking longer.
In the jaw specifically, muscle pain and fatigue as a result of stress-driven daytime clenching and night grinding can be impactful and persistent
Men can experience this as well, but women tend to develop more sustained symptoms, which increases the overall load on the system.
The Emergence of TMJ Symptoms
In our NYC metropolitan area practices, we commonly see TMJ symptoms develop as a result of a specific traumatic event, a mind-body disorder that drives persistent muscle tension, or an underlying medical condition that reduces tissue resiliency in the jaw muscles and temporomandibular joints.
Sometimes multiple factors are responsible, and symptoms develop gradually.
First, the body adapts. Then it begins to struggle. In women, as a result of the biological factors mentioned, the likelihood of a TMJ problem emerging and hanging around increases. At times, TMJ symptoms such as jaw pain, clicking, locking, tightness, frequent headaches, or facial pain no longer resolve on their own but require explanation and formal treatment.
A More Complete Understanding for Women
Biological vulnerability is real, but it does not mean that tissue healing and feeling better are not achievable. With the right evaluation, the causes and risk factors can be addressed comprehensively with education and a wide variety of supportive treatments that lead to meaningful and sustainable improvement.
Are You a Woman Experiencing TMJ Symptoms in the NYC Metropolitan Area?
If you are dealing with persistent jaw pain, clicking, locking, tightness, frequent headaches, or facial pain, there is a reason why.
At New York TMJ & Orofacial Pain, we specialize in diagnosing and treating TMJ disorders and orofacial pain. We take the time to understand what is actually driving your symptoms and build a treatment plan around it.
Our team of orofacial pain specialists provides evidence-based, individualized care at our locations in the NYC metropolitan area. We work closely with each patient and often other healthcare providers to restore comfort and function.
If your symptoms have persisted despite reassurance or prior treatment, a more specialized evaluation can make all the difference.
About Our Practice →
Treatments We Provide →
Read: Women & Pain →