In a recent episode of “Fit as a Fiddle,” I had the privilege of discussing a subject that has been the focus of my career with host Dr. Sneha Gazi. Temporomandibular Disorders (TMD) represent a complex and often misunderstood group of conditions. My colleagues and I at New York TMJ and Orofacial Pain are dedicated to unfolding the layers of TMD and providing relief to those afflicted.
Understanding the Orthopedic Complexity of TMD
TMD is not just about dental health; it’s an orthopedic issue that involves the musculoskeletal system of the jaw. Much like conditions affecting the knees, hips, or ankles, TMD requires a detailed understanding of the anatomy and function of the jaw. Distinguishing between the various causes of TMD symptoms—be it muscle tension, tendon issues, or joint dysfunction—is critical for effective treatment.
The Crucial Role of Diagnosis
A cornerstone of our discussion centered around the vital importance of accurately diagnosing TMD. With symptoms ranging from pain to limited jaw movement or even audible mechanical noises, the precise source needs careful identification. This emphasis on diagnosis not only guides our treatment approach but also helps the patient understand their condition better.
Emphasizing Patient Participation in Treatment
In my experience, successful treatment of TMD hinges on the active participation of the patient. The journey to recovery is a shared one, requiring changes in daily habits, posture, diet, and stress management. By engaging in their health and treatment plan, patients can significantly influence their outcomes, heralding a more effective and lasting relief.
Beyond Traditional Treatments: A Holistic Approach
While traditional treatments like oral appliances, muscle and joint injections and medications play a role in managing TMD, they are but a part of the holistic approach we advocate. The inclusion of lifestyle adjustments, reduction of daily jaw overuse behaviors and neck posture fatigue along with management of life stressors remains vital.
Closing Thoughts: A Path Forward for TMD Patients
As we concluded our conversation on the “Fit as a Fiddle” podcast, the overarching message was one of hope and optimism. TMD, with its multifactorial nature, requires a concerted effort both from the healthcare provider and the patient. Together with my colleagues at New York TMJ and Orofacial Pain, we stand ready to guide patients through their journey to recovery, using a comprehensive and empathetic approach. Here, you’re not just a statistic but a participant in a shared quest for understanding, relief, and recovery.
We have four locations in the New York City metropolitan area staffed by experienced and caring board-certified Orofacial Pain specialists who will correctly diagnose your condition and create a treatment plan to help you feel better. Please call us to schedule a consultation at your nearest location (see below). If you live outside the NYC area, the American Academy of Orofacial Pain’s directory will help you find an Orofacial Pain specialist in your area.
Remember, the path to overcoming TMD is a collaborative venture, and you are not alone.
In the intricate workings of the human body, few conditions are more intertwined with biology, psychology, and neurology quite like TMJ (temporomandibular joint) disorders. As someone deeply entrenched in the study and treatment of TMJ disorders for over 4 decades, I’ve seen firsthand the disproportionate impact these conditions have on women.
At our practice, New York TMJ & Orofacial Pain, 77% of our patients are women. This figure intriguingly spikes to almost 90% among those opting for BOTOX® injections to combat severe jaw muscle pain.
Not Mere Statistics
These numbers are more than mere statistics; they help Orofacial Pain specialists like us understand gender-specific vulnerabilities and design targeted, effective treatments for our female patients. The research that’s been done into this gender bias has primarily focused on three areas:
The Influence of Estrogen
Psychological Factors
Neurological Factors
Estrogen’s Critical Role
Estrogen has a critical role in reproductive health, but it also wields significant influence over TMJ symptoms. Fluctuations in estrogen levels punctuate women’s life events from menstruation to pregnancy to menopause. However, most people don’t know that these fluctuations can have a significant impact on the severity of TMJ symptoms.
This hormonally fueled modulation of pain perception and inflammation, coupled with its impact on ligament elasticity, intricately ties a woman’s hormonal rhythms to the functionality of their jaw joints.
Menstruation, Menopause, & Hormone Therapy
Estrogen levels fluctuate during menstruation, menopause and for those using hormone replacements or birth control pills, potentially making pain more pronounced. Many patients tell us that during the week leading up to menstruation and during menopause, they experience increased TMJ pain and dysfunction. Estrogen also reduces the strength of ligaments, making the ligaments in the jaw structure more flexible, which can cause injury to the TMJs. Jaw overuse behaviors such as awake or sleep bruxism, chewing gum, nail-biting, cuticle biting, and the like cause more TMJ dysfunction in women than in men.
Pregnancy’s Unique TMJ Challenge
During pregnancy, a woman’s body releases Relaxin, a hormone that prepares the body for childbirth (a good thing) but can intensify or trigger TMJ problems. This underscores the need for nuanced, compassionate care strategies that resonate with the body’s unique hormonal landscape during pregnancy.
The Mechanics of Muscle Fatigue
Jaw muscles respond to stress and strain in a unique way. Overuse behaviors can quickly fatigue them, producing lactic acid that causes pain and spasms. Moreover, the flexibility of the muscles, a trait more pronounced in women, may also be linked to jaw hypermobility – a common precursor to TMJ problems.
The Neurological Perspective
Finally, groundbreaking research has revealed that men and women process pain differently. Brain imaging techniques show differing patterns of brain activation in response to pain between women and men. Women have significantly lower pain thresholds than men and, therefore, typically seek care for TMJ-related symptoms more quickly. This spotlights the critical need for gender-aware TMJ specialists.
The Road Forward
It’s obvious why TMJ disorders disproportionately affect women. This knowledge enriches our practice’s understanding and cements our commitment to fostering hope and healing for women and everyone.
If you or someone you know is suffering, look for care at a practice that appreciates the gender-specific nuances of the experience.
Conclusion
At New York TMJ & Orofacial Pain, we provide compassionate, empathetic, and personalized care for people suffering from the often devastating effects of TMJ problems. Here, you’re not just a statistic but a participant in a shared quest for understanding, relief, and recovery.
We have four locations in the New York City metropolitan area staffed by experienced and caring board-certified Orofacial Pain specialists who will correctly diagnose your condition and create a treatment plan to help you feel better. Please call us to schedule a consultation at your nearest location (see below). If you live outside the NYC area, the American Academy of Orofacial Pain’s directory will help you find an Orofacial Pain specialist in your area.
Every day, you wake up with a pounding headache in your temples. It’s been going on for months. In an attempt to identify what’s causing your headaches, you jump online and come across more than a few web pages that suggest they could be caused by nighttime teeth clenching, also called Night Bruxism.
I’m John Dinan, an Orofacial Pain specialist practicing in the New York City metropolitan area. Orofacial pain is a dental specialty that helps people suffering from unexplained pain in their head, face, or neck.
Identifying the Cause: Teeth Clenching or More?
Morning headaches can indeed be related to nighttime teeth clenching, particularly if your pain is felt in the sides of your head. Here’s why: Your temporalis muscles, which cover the sides of your head up to the edges of your eye sockets, allow your jaw to open and close. When you clench your teeth for hours every night, your temporalis muscles can become very sore, resulting in pain in your temples when you wake up.
Other Contributors to Morning Headaches
Not every morning headache is caused by teeth clenching. There are dozens of conditions that can result in morning headaches. So, it’s essential to rule out other possible causes before scheduling an appointment with an Orofacial Pain specialist.
Poor Sleep : Sleep is essential to health, and according to the American Academy of Sleep Medicine, adults should get at least 7 hours of sleep per night. Sadly, most people simply do not allow themselves enough time for sleep, and this lack of sleep over time can lead to health problems such as cardiovascular disease, depression, diabetes, and pain.
Sleep hygiene best practices include going to sleep at the same time every night, making sure your bedroom is quiet, dark, relaxing, and a comfortable temperature, removing electronic devices from the bedroom such as TVs, computers, and smartphones, avoiding large meals, and drinking caffeine or alcohol before bedtime.
Migraine : Migraines are characterized by recurrent, often disabling, headache attacks and affect about 12% of Americans. Many people who get migraines go to bed feeling fine but wake up with a throbbing headache, sensitivity to light and sound, and nausea.If your morning headaches sound like this, you may have a migraine condition. Happily, migraines can be successfully treated by your primary care provider or a neurologist.
Alcohol & Caffeine : A typical alcohol hangover is characterized by a wicked headache the next morning. However, caffeine withdrawal symptoms can cause morning headaches, too. Within 24 hours of having your last cup of coffee, your body may start to experience withdrawal symptoms, including headaches upon awakening, as the effects of yesterday morning’s coffee wear off. And, of course, many illicit drugs have withdrawal side effects, including morning headaches.
If you suspect alcohol, caffeine, or other drugs may be causing your headaches, it’s time to reduce or stop and see if they subside.
The ‘Headache Bucket’ Theory : Envision a metaphorical bucket representing your capacity for headaches. Various elements contribute to this ‘headache bucket’ — including poor sleep, migraines, and sleep bruxism — each adding to the overall burden. When your bucket overflows, you experience a headache. It’s important to realize that even if sleep bruxism isn’t the primary issue, it could still play a significant role in amassing the volume that leads to your pain.
Moving Forward: Steps to Alleviate Your Pain :
Let’s confront these causes together. When other potential reasons have been excluded or are being managed, yet the headaches persist upon waking, it’s time to consult an Orofacial Pain specialist. If teeth grinding emerges as a contributory factor, rest assured, there is a suite of effective treatments on hand, ranging from conservative self-care approaches to sophisticated therapeutic interventions.
Taking Action: Don’t Let Headaches Hold Your Mornings Hostage :
The pathway to alleviating your morning headache lies in a proactive approach—explore each cause, seek professional advice, and embrace the treatments that resonate with your needs. Reflect on your sleep habits and substance intake, and consult a specialist for personalized guidance.
Dr. John Dinan, DMD MS is a board-certified Orofacial Pain specialist at New York TMJ & Orofacial Pain.
If you live in the NYC metropolitan area and are suffering from TMJ symptoms, feel free to contact us and make an appointment to see one of our Orofacial Pain specialists.
There’s a good chance you landed here because you’ve been suffering from an unexplained toothache, a persistent sinus pain that won’t leave you alone, or an annoying earache that makes you wince every time you chew for a long time. These symptoms have likely sent you on multiple visits to healthcare professionals, each one leaving you with more questions than answers.
But what if the source of your pain is not where you’re feeling it?
Your puzzling array of symptoms just may be due to problems with your temporomandibular joints (TMJs) and associated muscles. Your TMJs and jaw muscles play a fundamental role in the basic movements of your jaw—talking, chewing, yawning, and even expressing emotions. When this joint and its corresponding muscles and ligaments become strained, unstable, and or overworked, the resulting condition is known as temporomandibular disorder or TMD.
When a TMD problem is not considered as a source of pain in teeth, the ear and/or sinus, for example, the result can be ongoing evaluations and treatments that address the location of the pain symptoms but not the origin. When the location of the pain complaint is not the true origin, the term referred pain is commonly used.
Referred Pain & Its Relationship To TMD Problems
Referred pain is pain perceived at a location other than the origin of the painful stimulus. It is the result of a network of interconnecting sensory nerves that are persistently over-excited. For example, when there is an injury or pathology at one site in the network, it is possible that when the signal is interpreted in the brain, mistakes are made as to the true origin of the problem. As a result, pain is often experienced at a distance from the true origin. (E.g., pain from a heart problem is experienced in the shoulder or jaw)
So, how does this relate to the structures of the jaw?
When your jaw muscles (masseters and temporalis) are persistently overworked, they become sore, extremely sensitive, and knotted. These areas are known as trigger points. When activated, trigger points can send pain signals to places far from their origins, resulting in referred pain. Jaw overuse behaviors such as clenching your teeth during the day, biting your nails, chewing your pens, etc., can lead to the formation and activation of these trigger points, leading to referred pain in areas such as your teeth, ears, or sinuses.
Referred Pain to the Teeth, Ear, Sinus, and Face from the Masseter MuscleReferred Pain to the Teeth, Ear, Sinus, and Face from the Temporalis Muscle
Orofacial Pain Specialists Understand What You’re Going Through
As part of an Orofacial Pain practice, my colleagues and I are well-versed in the nuances of this disorder. For many of our patients, merely validating their pain and helping them understand the concept of referred pain gets them moving in the right direction on the road to recovery.
If you’re nodding your head right now, thinking, “That’s me!” I encourage you to seek the care of an Orofacial Pain specialist. Your treatment plan might include education, awareness strategies to reduce jaw overuse behaviors and fatiguing postures, oral appliances, exercises, and/or relaxation techniques to address daily worries and stress. In addition, physical therapy can also be helpful, along with muscle injections, to break up the trigger points that are driving your pain.
How To Get Help Now
If you live in the NYC metro area and are ready to uncover the root of your Orofacial Pain, we are here to guide you. Take the first decisive step by scheduling a consultation at one of our convenient offices in Manhattan, White Plains, New Jersey and on Long Island. Together, we’ll get to the bottom of what’s causing your suffering and get you on the road to recovery.
As a board-certified Orofacial Pain specialist, I focus entirely on caring for patients who suffer from facial and unexplained tooth pain. Every week, I see someone in our office seeking our help. Sometimes, the problem is they still have a toothache after a root canal, and the reason why has been unclear.
Before I get into what can cause a toothache after a root canal, let’s discuss what a root canal is in the first place. A root canal is a dental procedure to remove inflamed or infected nerve tissue on the inside of a tooth. The compromised nerve tissue or pulp is removed, the space occupied by the pulp (the canal) is carefully cleaned and disinfected, and then the empty canal space is filled and sealed.
Root canal treatment is designed to eliminate inflamed or infected pulp tissue, removing bacteria at the same time. When accomplished properly, reinfection is unlikely, and the tooth will remain asymptomatic and stable.
Around 95% of patients who have a root canal never again feel pain in the treated tooth. But what happens to the 5% of people who still have a toothache after a root canal? If that’s you, you’re in the right place.
Did This Happen To You?
One day, you woke up with a terrible toothache. You took some Ibuprofen and powered through your day. But you were still in pain a few days later. So you see your dentist, who tells you, “You need a root canal.”
You weren’t excited about having a root canal, but you were looking forward to your tooth pain being a thing of the past. But that’s not what happened.
Your pain persisted for another week, so you went back to your dentist, who told you: “Everything looks good. Try to be patient while it heals.” But the pain never went away. What’s going on?
Before I go any further, I want to emphasize this:
If your dentist recommends a root canal after a thorough examination and x-rays, don’t resist! Remember, 95% of root canals are completely successful. In the rare cases when they’re not, one of these three scenarios likely holds the explanation:
3 Common Causes Of Persistent Toothache After A Root Canal
Scenario 1: The root canal was necessary, but it didn’t get rid of your toothache
Under this scenario, your dentist accurately diagnosed the cause of your toothache and appropriately recommended root canal therapy. However, your pain persists.
At this point, your dentist may send you to an endodontist to take a look. Endodontists are root canal specialists who typically have advanced diagnostic tools in their offices, such as 3D cone beam imaging and highly magnifying operating microscopes.
The endodontist will look for clues to explain why you still have a toothache. They may detect a crack in your tooth that wasn’t visible in the x-rays at your dentist’s office. Or they find a lingering infection that needs to be removed in a curved part of the root that wasn’t fully cleaned the first time. Or, there may be another canal that needs to be treated that hadn’t been detected.
If this is your scenario, you’re in luck! You may have to endure a bit more time in the dental chair, but your pain will resolve, and your life will go on.
Scenario 2: The root canal was necessary, but a different kind of pain emerged
You may have heard about a strange phenomenon called phantom limb pain. Phantom limb pain is when someone who has lost a limb still feels pain in the limb, even though it’s gone! A similar thing can happen in dentistry when pain continues to be experienced in a tooth after the nerve tissue and pulp that we mentioned above are removed.
Fortunately, the incidence of phantom tooth pain after a root canal is much lower than that of phantom limb pain after an amputation. In both cases, however, research has suggested that, at times, removal of dental pulp can cause a nerve injury that leads to persistent pain. The formal term for phantom tooth pain is Post Traumatic Trigeminal Nerve Pain or PTTNP. The trigeminal nerve is the cranial nerve responsible for sensations in teeth.
Unfortunately, there can be a delay in making this diagnosis because your previous exams and x-rays suggest there’s nothing wrong despite your pain. Your frustration understandably grows as you can end up feeling that, somehow, it’s your fault.
At this point, your dentist or endodontist might refer you to an Orofacial Pain specialist like the doctors at our practice. Orofacial Pain specialists have advanced training in diagnosing and treating unexplained toothaches and fully understand the complexities of trigeminal nerve pain. The education and care they can provide with oral and topical medications are often the first steps toward pain relief.
If a referral to an Orofacial Pain specialist isn’t suggested – ask!
Scenario 3: It turns out your root canal wasn’t necessary
Before you read on, I can’t express this enough: 95% of root canals are necessary and successful!
But occasionally, a non-tooth-related condition can cause pain that mimics a bad toothache, and no amount of root canal therapy will help. It may be hard to appreciate, but your toothache from day one may have been caused by something that didn’t originate in your tooth. As a result, the root canal failed to get rid of the pain.
Less obvious causes for a lingering toothache after a root canal is referred pain from your jaw muscles. When these muscles become fatigued from constant bruxism or fatiguing head posture, it can actually cause pain in a tooth. As Orofacial Pain specialists, we commonly see patients who were diagnosed with a TMJ problem or a chronic neck problem and report persistent tooth pain. Nearly 18% of the population suffers from a TMJ disorder, so this scenario is commonly seen in our practice.
Thankfully, we have strategies to get rid of that lingering tooth pain. Treatment can be a combination of strategies that include changing daytime jaw overuse behaviors and fatiguing head postures, exercises, medications, muscle injections, and custom oral appliances.
There can be other medical causes of persistent toothaches. They are rare but should be mentioned: Lyme disease, cardiovascular problems, sinus infections, salivary gland pathology, trigeminal neuralgia, and intracranial diseases inclusive of brain tumors. Orofacial Pain specialists have been trained in very specific ways to listen to the symptoms and stories of pain, looking for clues to make alternative diagnoses or referrals to medical colleagues to broaden out the evaluation process.
In Conclusion
If you have a lingering toothache after a root canal and neither your dentist nor an endodontist can figure out why, request a referral to an Orofacial Pain specialist.
If you’re located in the NYC metro area, we have offices in Manhattan, White Plains, Long Island, and New Jersey. Click here for exact locations and contact info.
Outside our area? Check the directory of the American Board of Orofacial Pain for a specialist in your area with Diplomate designation.
Dr. John E. Dinan is a Diplomate of the American Board of Orofacial Pain and the American Board of Dental Sleep Medicine. He is part of the team at New York TMJ and Orofacial Pain team, practicing in our Manhattan and Springfield, NJ offices.
If you’re one of the millions of people who suffer from persistent jaw pain and unexplained headaches, there’s a good chance your dentist has diagnosed your condition as TMD (temporomandibular joint disorder). But when the treatments that work for most people, such as oral appliances, exercises, and relaxation techniques, don’t work for you, your symptoms may stem from an entirely different condition.
I’m Dr. John E. Dinan, one of the board-certified Orofacial Pain specialists at New York TMJ & Orofacial Pain. Orofacial pain specialists like me focus on the needs of patients who have jaw disorders, persistent toothaches, nerve pain disorders, and headaches – what most people call TMJ.
For years, patients have come to our practice having been diagnosed with TMJ pain and disorders only to discover they were facing something entirely different – migraine. Let me tell you about two such patients whom I’ll call “Nora” and “Veronica.”
Nora’s Story
Nora, 36, had been living with pain for over two decades. Every month during her menstrual cycle, she experienced excruciating and throbbing pain in her right temple and jaw. These episodes brought with them heightened sensitivity to light and sound. She told us that the pain was so awful that it actually made her nauseous.
Nora’s agony lasted for 48 to 72 hours before it finally subsided, only to return the next month. She also heard a clicking sound in her right temporomandibular joint (TMJ) when she opened her mouth wide. Nora had been diagnosed with TMJ many years before coming to our office. Numerous types of oral appliances gave her no relief. The only thing that helped was Ibuprofen, but it only reduced her pain by about half.
When we reviewed her dental records and x-rays, we discovered that her jaw and temporomandibular joint were normal.
Veronica’s Story
Veronica, 24, arrived at our office, also having been diagnosed with TMJ. For five years, she had experienced severe throbbing pain two to three times every month in front of her right ear and under her right eye. Like Nora, Veronica’s dental records and x-rays showed no definite jaw issues. Unlike Laura, her pain was not accompanied by jaw clicking.
Veronica’s pain episodes typically lasted between 24 and 48 hours and were accompanied by heightened sensitivity to light and sound and periods of nausea.
How We Arrived At Our Diagnosis
At our practice, the method of diagnosis is focused first on listening carefully to our patients’ stories. Next is a comprehensive medical and dental history assessment and an examination and imaging.
In the end, it was apparent that both patients did not have TMJ; they had migraine. The misdiagnosis had led to ineffective treatments and endless suffering.
Symptoms Of Migraine
Migraine affects about 12% of the population and is characterized by a combination of the following:
Moderate-to-severe pain intensity
Pain that pulses
Gets worse from physical activity
Includes nausea and/or vomiting
Sensitivity to light and sound
Pain periods from four to 72 hours
About a third of migraine sufferers also experience visual, auditory, and sensory changes right before a migraine.
When we compared Nora’s and Veronica’s symptoms to the list above, it confirmed our suspicions: the issue was migraine, not TMJ.
Next, Treatment
Both patients were ecstatic when we explained to them that they experienced migraine, and it is treatable. After years of their lives disrupted by pain, they finally could see a light at the end of the tunnel. We prescribed sumatriptan, a medication known to alleviate migraine-related symptoms such as nausea, vomiting, and light and sound sensitivity. Some patients discover their migraines vanish entirely, and others find their symptoms less intense with sumatriptan.
Great News!
Nora and Veronica both got relief from their pain attacks with sumatriptan (which further confirmed the diagnosis of migraine). They now see their primary care physician for their long-term management and prescriptions.
From a doctor’s point of view, it is a great joy to see patients emerge from the disabling impact of chronic pain. Nora’s and Veronica’s stories highlight the importance of an accurate diagnosis. While we couldn’t change the past, we opened the door for them to have a brighter future.
Conclusion
If you can relate to Nora’s and Veronica’s stories and live in the NYC metropolitan area, feel free to reach out to us. We’re here to listen to you and help you on your journey to getting relief. Click here for our office contact information.
If you’re outside the NYC region, you can locate an Orofacial Pain specialist in your area by going to the American Board of Orofacial Pain directory. Click here.
If you’ve been dealing with frustrating and sometimes debilitating ringing, buzzing, or humming in your ears and haven’t been able to find relief, it’s time to consider the possibility that your temporomandibular joints (TMJs) are playing a role. As Orofacial Pain specialists, we’re experts at dealing with jaw-related problems. We understand your challenges and how they could be negatively affecting your life, and we’d like to provide you with some clear and understandable information that can help you determine if TMJ is involved with your symptoms.
You’re Not Alone.
According to a 2022 systematic review published in the Journal of the American Medical Association (JAMA), more than 740 million people worldwide experience tinnitus. The National Institute on Deafness and Other Communication Disorders (NIDCD) estimates that over 25 million Americans (10% of the U.S. adult population) suffer from some form of the condition.
Here’s How Tinnitus and TMJ Can Be Linked
Tinnitus is defined as the perception of sound that doesn’t have an external source. It is most likely to affect people ages 45 years old and older. And, while tinnitus can have various causes – such as noise exposure, medication use, infections, and even head trauma – there’s a lesser-known possibility: a connection between tinnitus and TMJ.
An intricate relationship between your ears and jaws sheds light on the possible connection between tinnitus and TMJ. Specific structures in our ears and jaws develop simultaneously from similar tissues, which has led researchers to believe that issues with temporomandibular joints and the muscles and ligaments that control them, may have an effect on the ears and contribute to tinnitus symptoms.
Is Your Tinnitus Linked To TMJ? – 5 Questions
To determine if your tinnitus symptom TMJ may linked to TMJ, answer these 5 questions:
Does the intensity or character of your symptoms change from one day to the next?
Do your symptoms change when you open or close your mouth or move your jaw forward or back?
Does chewing food affect the intensity of your tinnitus?
Do your tinnitus symptoms change when you clench your teeth?
Do your symptoms worsen when you turn or tilt your head?
What To Do Next
If you answered yes to one or more of the above questions, we have some good news for you: There is hope for relief! Here’s what to do next:
Step 1: Rule out any serious medical conditions that could be contributing to your tinnitus. If you haven’t been seen by an Ear, Nose and Throat (ENT) doctor, make that appointment first.
Step 2: Look for a board-certified TMJ and Orofacial Pain specialist in your area (instructions below). The field has been growing rapidly since the addition of Orofacial Pain to the list of specialties approved by the American Dental Association in 2020.
Board-certified orofacial pain specialists like the professionals at our practice have dedicated their careers to helping patients who suffer from the effects of TMJ. We have completed advanced training, have many years of experience, and attend courses to stay on the cutting edge of new research and treatment.
When a specialist evaluates a patient, no stone is left unturned to determine that best treatment plan. We take into consideration the patient’s medical and dental history and ask what’s going on in their life. Why do we want to know what’s going on in a patient’s life? Because it is believed that stress can lead jaw over-use behaviors, such as teeth grinding and clenching.
Your treatment plan may include one or more of the following:
Behavior Changes: Here, you become aware if you are grinding or clenching your teeth during the day, then work to reduce the daytime over-use behaviors so your jaws can relax.
Exercises: Special jaw exercises designed to stretch your muscles can help alleviate symptoms.
Physical Therapy: Many physical therapists are now trained in techniques to manage and reduce TMJ symptoms.
Oral Appliances: Also called mouthguards or teeth protectors, oral appliances are beneficial to reduce the effect of teeth grinding that can contribute to symptoms.
If you’ve been suffering for a while and are under the care of an ENT, you may be using approaches such as sound therapy. The treatments above work in tandem with other treatments, and new methods, including deep brain stimulation and repetitive transcranial magnetic stimulation, show hopeful promise for the future.
Conclusion: The Tinnitus Link To TMJ Should Not Be Overlooked
The possible connection between your tinnitus symptoms and TMJ should not be overlooked. Now that you understand the intricate relationship between jaws and ears and have answered the 5 key questions above, you’re ready to take proactive steps toward finding relief. You don’t have to be alone on this journey; solutions are within reach, and the care of an Orofacial Pain Specialist could be the turning point you’ve been waiting for.
To find an Orofacial Pain specialist in your area, search by city or state here: American Academy of Orofacial Pain. Look for a member that has “Diplomate” status
If you live in the New York City metropolitan area, New York TMJ & Orofacial Pain has a location near you. To make an appointment, click here.
If you’re suffering from painful jaw problems and are looking for the best treatments for TMJ, this article is for you. I’ve been a TMJ and orofacial specialist for many years, and I want to share some useful tips with you that help my patients feel better.
Start Here
For even the best treatments for TMJ to be successful, it’s crucial to try and understand the reasons why you have jaw problems in the first place.
Over the years, we have come to recognize that a significant number of TMJ problems occur as a result of the jaw muscles and temporomandibular joints being overworked. Since TMJ problems are essentially orthopedic problems in the jaw, daytime jaw over-use behaviors such as chewing gum, biting your nails or cuticles, clenching your teeth, bracing your jaw muscles, cheek and lip biting, or gnawing on non-edible items can all fatigue the jaw muscles and sprain the TM joints.
The origin of these daytime jaw overuse behaviors, however, can be rather complex and, as a result, often difficult for patients to change.
The Key Is To Stop Injuring Your Jaw Muscles and Joints
It seems like a no-brainer, right? Just stop your jaw over-use behaviors, and your TMJ problems will disappear. I wish it were that simple.
It requires a tremendous amount of focus and effort to stop behaviors that have likely been in your life for years and may even be comforting in times of stress. Just stopping these behaviors may not be sufficient to ease symptoms of pain and jaw clicking if the jaw muscles or joints have already been persistently injured.
In addition, the way you hold your head can increase the risk of developing a jaw problem. If you work at a computer all day or use your cell phone for hours a day, the position of your head could fatigue your neck muscles leading to jaw pain and even limited jaw motion. Remember, your head is heavy – and when it is forward, the neck muscles are put under strain leading at times to jaw problems.
Reducing or eliminating these behaviors and postures is, therefore, an important part of the getting better process, but achieving these changes takes time. While you’re working on that, I’d like to share with you the treatments we rely upon in our practice to help our patients heal and get better.
What Are The Best Treatments For TMJ?
The best treatments for TMJ always start with an accurate diagnosis. Not every pain in the face and jaw is due to a TMJ disorder. In fact, the broad term Orofacial Pain is now used to describe any discomfort or pain in the mouth, face, and neck region, including the jaw joint (temporomandibular joint or TMJ), muscles, teeth, and nerves.
In 2021, Orofacial Pain was designated as a recognized specialty within dentistry, and as a result, research relating to TMJ disorders will receive additional attention and funding.
Today we design treatment plans based on current research and what we learn from our patients – their medical and dental history and, most importantly, what is going on in their lives.
On a daily basis, there are several TMJ treatments that we rely upon that help the majority of our patients feel better and get better. They are:
Exercises – We frequently prescribe jaw and neck exercises to ease jaw/neck tension, stretch overworked muscles, and help them heal.
Physical Therapy/Chiropractic Care – If your TMJ symptoms have lingered for months or even years, a short physical therapy or chiropractic care regimen can help break the cycle of jaw muscle tension.
Oral Appliances – There’s a misconception that oral appliances (nightguards, mouthguards, bite plates, etc.) stop nighttime tooth clenching and grinding. They don’t. But what they can do, when designed correctly, is reduce the impact of clenching and grinding forces and limit potential injury to the jaw muscles and TM joints.
Medications that address pain, spasms, muscle tension, and inflammation.
Trigger Point, Prolo Therapy & Steroid Injections – Some of the best treatments for TMJ disorders involve injections that address pain, spasms, muscle guarding, soreness, and inflammation.
Trigger Point Injections and Dry Needling can be highly effective in breaking up stubborn knots in the jaw/neck muscles. In both cases, a few injection sessions are necessary for full benefit.Prolo Injections, which are a combination of local anesthetic and dextrose, are often used to reduce inflammation in tendons, ligaments, and joint capsules but have been shown to assist in tissue regeneration as well.Steroids still play an important role in reducing inflammation in the TM joints and supporting tendons and ligaments.
BOTOX® & Xeomin – BOTOX® and Xeomin are injectable neuromodulators that can ease muscle pain, tension, and nerve pain. These neuromodulators are commonly used in our practice, surrounded with ongoing education as to what these injectables can achieve, their limitations, and potential side effects.
Conclusion & Recommendations
If you’ve been suffering from persistent TMJ symptoms and live near one of our four offices in the NYC metropolitan area (Manhattan, White Plains, Long Island and New Jersey), give us a call at 212-265-0110 to set up a consultation.
If you live outside our area, try to find a board-certified Orofacial Pain specialist in your area. Ask your dentist for a referral or check the American Academy of Orofacial Pain’s directory and search for a specialist with Diplomate status.
You don’t have to live with pain forever. Help is here!
Suffering from TMJ pain? You’re not alone. Nearly 18% of the population suffers from a TMJ disorder, too. As a TMJ and Orofacial Pain specialist with over four decades of experience, I’ve helped thousands of people get relief from their pain and acquire control over their TMJ problems.
The symptoms of TMJ pain can be very different from person to person. For some, the pain is sporadic. For others, it lingers. Some people can’t open their mouths without intense pain; some suffer from severe headaches. TMJ pain is usually described as dull, aching, and sore. And many patients say their TMJ problem has taken over their life.
The #1 Reason For TMJ Pain Is Overworked Jaw Muscles
I’m happy to say most people do get better. The most important element of your TMJ treatment, and where we always start, is for you to unravel the mystery behind your TMJ pain.
The clue to your TMJ pain is found in your masseter and temporalis muscles, which are your jaw muscles. Your jaw muscles react to being overworked the same way as any other muscle – when they are overworked they can get sore, stiff, and achy.
For example, when you work in your garden for many hours on a Saturday, your back muscles are probably going to be sore and achy on Sunday. When you work out intensely at the gym, your muscles can ache. If you lift and carry your baby or toddler, you know how painful your arm, shoulder, and back muscles can be.
Your masseter and temporalis muscles are just as susceptible to overuse and fatigue as your back, legs, shoulders, and arms. So, what causes jaw muscles to become overworked? The most common reasons for jaw tension are continuous daytime jaw over-use behaviors, such as:
Teeth grinding and clenching
Gnawing on pens
Chewing gum
Biting your nails or cuticles
Biting your lips or the inside of your mouth
But there’s something behind the persistent muscle tension that just may be the cause of your TMJ pain…
Your TMJ Pain May Well Be Tied To Your Emotions
It may seem strange to tie your jaw muscle problems to your emotions. But over the years, TMJ specialists began to notice some stark similarities among their patients. They discovered that the majority were living lives filled with negative emotions such as constant stress and worry. Many were dealing with a serious illness, unrelenting pressure at work, caring for an aging parent, or having marital problems, to name a few.
Negative emotions that come from constant stress and worry can lead to what I like to call “an upset brain.” An upset brain can lead to persistent muscle tension, which can then trigger daytime jaw over-use behaviors such as the ones I listed above.
Constant stress and worry can harm the quality of sleep, as well. An upset brain can trigger nighttime teeth clenching or grinding, which overworks your muscles and often results in morning TMJ pain and stiffness.
The Link Between Overworked Jaw Muscles & Prescription Medications
There’s another possible reason you have TMJ pain. Many people rely on medications such as Adderall, Ritalin, Concerta®, and Vyvanse® to enhance their brain focus. While they’re effective, they can also stimulate your internal fight-or-flight system, which in turn can lead to jaw over-use behaviors, which in turn can cause jaw problems.
What To Do Next
TMJ and Orofacial Pain Specialists have a toolbox full of treatments to help people get in control of their TMJ so they can feel better, heal, and get their lives back. Treatments include behavior modification, relaxation and breathing strategies, exercises, medications, and oral appliances. Trigger point injections, prolo injections, and BOTOX® can be very effective as part of an overall treatment plan, as well.
Now that you are aware that the #1 reason you have TMJ pain is your overworked jaw muscles, it’s time to get help. Click here to learn more about the best treatments for TMJ.
Dr. Donald R. Tanenbaum
Are you located in the NYC metro area? We can help you. Our practice has four convenient locations: Manhattan, White Plains, Long Island (2 locations), and Springfield, NJ. To make your appointment, call 212-265-0110.
Patients will often come to me suffering from symptoms of TMJ and looking for solutions that don’t involve medication or surgery. Symptoms such as facial pain, headaches in the temples, inability to open to the mouth widely, sensitive teeth, or aching and throbbing jaw muscles can be unbearable. There are numerous remedies, for jaw related symptoms that include massages, home exercises, physical therapy, modified diets, and changes in daytime behaviors/postures. At times an oral appliance is an important part of care. These devices are commonly used for the treatment of TMJ problems and can be used in a number of different ways.
What is an oral appliance?
An oral appliance is a device that fits over your teeth with the intent of reducing tooth wear, tooth mobility, tooth sensitivity, muscle pain and soreness and joint pain and instability. At times but not frequently these devices are designed to “align the jaw.” They can also be used to discourage some of the daytime behaviors many patients don’t realize they’re doing, such as resting their teeth together, clenching their teeth, or biting their nails or cuticles. These appliances can be worn at night and/or during the day
In general the intent of these appliances is based on the problems experienced by patients.
Night guards: Most commonly these appliances are chosen by dentists to address tooth wear, soreness, and mobility that occur as a result of night clenching or grinding of the teeth. Many patients that develop tooth wear do not even realize that they have a problem and often deny grinding their teeth at night. These devices when used in patients without active symptoms (just wear of the teeth) don’t require much adjustment and should be brought by the patient when they return to the dentist for tooth cleaning visits. Typically these devices are custom fit so that they are retentive, not too thick, and modifiable over time. Over the counter devices sold in pharmacies and online are for the most part inadequate, as they are often too thick, poorly retentive, and inadequately cover all of the teeth. As a result these devices can often prompt more clenching, and/or allow tooth shift.
Night appliances to address TMJ problems: Based on the specific jaw problem that is diagnosed (muscle soreness, morning temporal headaches, limited jaw opening in the morning…etc) oral appliances at night are designed to reduce overuse and loading forces to the TM Joints and jaw muscles. The biting surface of the appliance is therefore designed and modified to most efficiently address the problems at hand. Most commonly the biting surfaces are flat but, at times, inclines and ramps are used to confront unstable joint ligaments and displaced discs. When used in patients with active symptoms, these appliances require frequent modifications requiring patient follow-up visits.
Day appliances to address TMJ Problems: At times there is necessity to have a patient wear an appliance during the day. For the most part these appliances are needed when there is extreme instability in a TM joint that has led to clicking, locking, and pain problems. These appliances are not worn all day and virtually never during chewing. At other times, oral appliances worn during the day hours can be used to get in the way of day behaviors and/or remind patients that during the day the jaw should be hanging in a rest position with the teeth apart.
How about oral appliances to re-align the jaw? This concept of jaw re-alignment to address a TMJ problem remains controversial. To date there is no science to support the concept that a poor bite or mal-aligned jaw is responsible for the emergence of TMJ symptoms. At most a bad bite or mal-aligned jaw may be a risk factor but with no more weight than other risk factors such as; female gender, gum chewing, clenching, night grinding, or stress. As long as there remain millions of people with bad bites and asymmetric jaws without symptoms this concept has to be viewed with skepticism. In addition, if an appliance were to be made to re-align the jaw, it would require the patient to bite or rest on it when in the mouth to hold the jaw in the ‘better’ position. This action of course would violate the principle that the jaws should hang at rest during the day. Clearly this option must be chosen with great care.
From an overall perspective the concept of curing a TMJ problem with an oral appliance is probably a bit of a stretch. Their use however is a critical part of TMJ treatment!
These appliances are extremely helpful in reducing the damage from night clenching or grinding. They work by diminishing the forces exerted on the TM joints and by diminishing the amount of contracture that can be generated in the jaw muscles. Night guards are most effective when custom fit, and adjusted over the course of time. Or you can purchase a generic set at a drug store. Obviously, custom-made night guards that have been conformed to your individual bite-print are more effective in treating TMJ symptoms, but the trade-off is that they’re more expensive.
Bite Splints: This form of therapy uses a mouth guard to physically correct the bite, rather than just relieve pain or reduce damage to the teeth. Bite splints are best for you if you have more extreme TMJ symptoms that need correcting in order to have a hope for any long-term relief. The primary difference between a bite splint and a night guard is that bite splints are worn around the clock, 24-7. It’s a full commitment to correcting the misalignment issues that are causing your TMJ.
So, can mouth guards cure your TMJ? The short answer is: Yes. In some cases, particularly with corrective bite splints, you can realign your bite over the course of time and eliminate those painful TMJ symptoms. In other cases, mouth guards can relieve your symptoms to the point where you feel very little pain or discomfort at all.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
You might have heard about the temporomandibular joint disorder (TMD), and this disorder is also called TMJ. If you have felt pain in your jaw, you might have this common condition. Or your dentist might have told you that you have it. If you have questions about it, keep reading to find out more.
About TMD
This is not just a single disorder. Instead, it is a group of several painful conditions. These affect the temporomandibular joint as well as the surrounding muscles. It is not known how many people have the condition. However, women are often affected more than men.
There are three main kinds of this condition. The most common type of TMD is myofascial pain. It is pain or discomfort in the muscles that work with the function of the jaw. It can also cause pain in the shoulder or neck muscles.
With internal damage to the joint, there might be a displaced disk. The condyle might be injured, or the jaw might be dislocated. With degenerative joint disease, the patient might have rheumatoid arthritis or osteoarthrosis. Someone might be able to have one or more of these conditions at once. Research is still being done on how physical, behavioral, and psychological factors might contribute.
Causes of the disorder
A severe injury to the joint might cause TMD. With a heavy blow, the bones can be fractured, or the disk can be damaged. That can disrupt the motion of the jaw and cause locking or pain. Arthritis can also develop after an injury.
In some cases, a bad bite might also trigger the condition. With orthodontic treatment, such as braces, TMD might be triggered. Some people believe that chewing gum can cause clicking sounds since the joint can be overused in that case. However, if there is only clicking, then the condition might not need to be treated.
Diagnosis of TMD
The symptoms and causes of TMD are still not known. That means that diagnosing them can be hard at times. Currently, there is no standard test that can identify the condition. However, the patient can usually describe the symptoms for a diagnosis. The physical examination will include:
Feeling the chewing muscles and joints for tenderness or pain
Listening for popping, grating, or clicking as the joint moves
Looking for jaw locking or limited motion while the mouth closes or opens
It is also important to look at the dental and medical history of the patient. Many times, this will give the provider enough information to find the source of the pain. Then the jaw problem or pain can be identified. The patient can then get treatment.
Visit a dentist for TMD treatment
If you have pain in your jaw, you might want to consider having a dentist look at your symptoms. If you do have a TMD disorder, then getting treatment can provide you with relief. That will also prevent long-term damage to your joint. Making an appointment today is your first step.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
CPAP alternatives are the industry’s best-kept secret. Do you suffer from sleep apnea? If so, then you are not alone. Sleep apnea can cause several health problems, and it is important to get the right treatment for your condition. Alternatives are an option that many patients don’t know about. This blog post will discuss what they are and how they work, providing information on why dental patients should consider them when choosing their next step in treating sleep apnea-related conditions.
What are alternatives?
CPAP stands for continuous positive airway pressure. It is the most well-known treatment option for sleep apnea sufferers, but it may not be the best choice. This type of machine uses air to help keep your airway open at night, so you don’t have to struggle to breathe. You wear it over your nose, and it is attached to a mask that fits around your mouth.
Alternatives are not machines but adjustable oral appliances. They work in the same way as CPAP; adjustable pressure keeps your airway open while you sleep so you can enjoy deep sleep without struggling for breath. They are worn over your teeth, much like a mouthguard used by athletes.
There are many pros and cons to both CPAPs and Alternatives, but dental patients should know that each can be effective in treating sleep apnea-related conditions. Let’s take a closer look at these alternatives so you can make an informed decision about what is best for your sleep and health.
Why should I consider CPAP alternatives?
Alternatives are not as cumbersome as regular CPAPs, so they may be a better option if you can’t handle wearing a machine over your nose all night long. They are also adjustable, unlike traditional machines that offer only one level of air pressure. Many people find the adjustable nature of these appliances to be a better treatment option because they can fine-tune them to achieve comfort and effectiveness with fewer side effects.
Patients with dental work may also benefit from using Alternatives. If you have a crown or other type of dental restoration, this type of machine may be preferable.
Alternatives are also far less expensive than the traditional CPAP machines, which is another reason why patients should give them serious consideration when deciding on treatment. Many insurance carriers will not cover the cost of a sleep apnea machine, but they might help pay for an oral appliance since full coverage can lower your long-term medical expenses.
What should I expect if I choose CPAP alternatives?
The first step is to see your dental sleep apnea specialist and get a proper diagnosis of your sleep apnea condition. Your dental sleep apnea specialist can then help you decide between alternatives and traditional CPAP machines. Dental patients often prefer the sleep appliance route because of its lower cost and adjustable design, which is tailored for comfort and effectiveness.
If you ultimately decide on an alternative, your dental sleep apnea specialist will fit you for the appliance. You can choose from a complete or partial device depending on your preference, but both are equally effective in treating sleep apnea-related conditions.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
This content was originally published on 2/9/2022 and reviewed on 6/19/2026.
When patients come to my office with the complaint of persistent (and often acute) pain in their face or jaw, they often fear they have a problem called trigeminal neuralgia.
Before discussing this specific type of facial pain, a brief discussion about the trigeminal nerve and its role in virtually all facial pain problems is essential.
The trigeminal nerve is but one of 12 cranial nerves that can transmit two types of information to the brain.
Sensory Information: Includes details about smells, sights, tastes, touch, sounds, and PAIN to the brain.
Motor Information: Initiates movement or activation of muscles and glands.
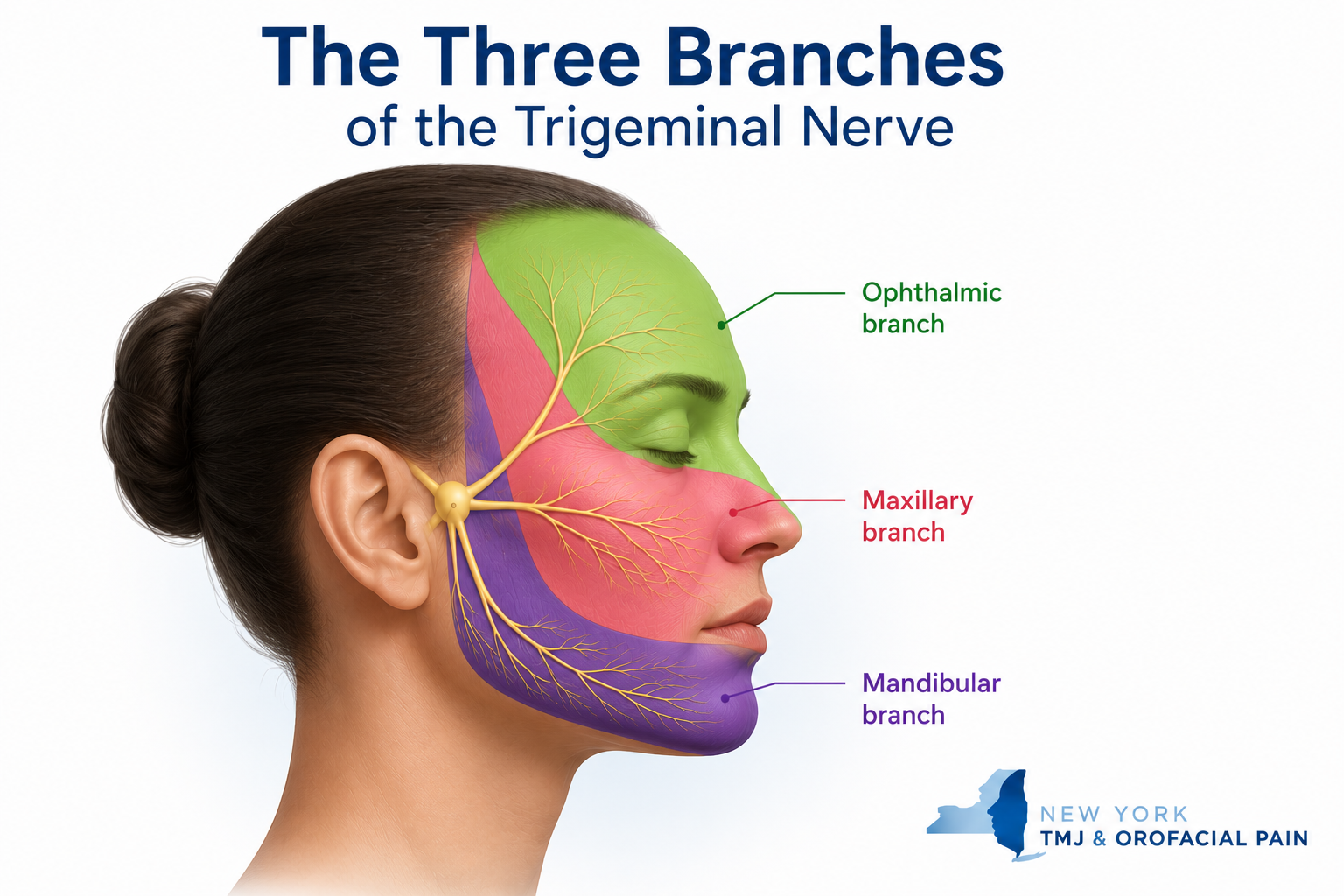
The Three Branches of the Trigeminal Nerve
The trigeminal nerve has three different divisions, each with a slightly different function:
The trigeminal nerve has three main branches: ophthalmic, maxillary, and mandibular, which carry sensation from different areas of the face, teeth, jaw, and mouth.
1. The Ophthalmic Division
The ophthalmic division transmits sensory Information to the brain from:
The scalp
The forehead
The upper sinuses
The upper eyelid and associated mucous membranes
The cornea of the eye
The bridge of the nose
2. The Maxillary Division
Like the ophthalmic division, the maxillary division of your trigeminal nerve has only a sensory component. It transmits sensory Information to the brain from:
The lower eyelid and associated mucous membranes
The middle part of the sinuses
The nasal cavity and middle part of the nose
The cheeks
The upper lip
The teeth of the upper jaw and the surrounding gum tissue and supporting bone
The roof of the mouth
3. The Mandibular Division
The mandibular division is the only part of the trigeminal nerve that has both sensory and motor functions. It communicates sensory Information to the brain from:
The outer part of the ear
The lower part of the mouth and the associated mucous membranes
The front and middle parts of the tongue
The teeth of the lower jaw and the associated gum tissue and supporting bone
The lower lip
The chin
The temporomandibular joint and jaw muscles
The mandibular division also stimulates movement of the muscles in the jaw and some of the muscles within the inner ear.
What Is Trigeminal Nerve Pain?
As a result of the trigeminal nerve’s sensory function and broad distribution in the intraoral tissues, facial and jaw structures, the majority of all orofacial pain is due to excitation, irritation, and or injury to the trigeminal nerve.
Common toothaches, wisdom tooth pain, dental infections, sinus pains, jaw muscle pain, and temporomandibular joint pain all involve the trigeminal nerve. Therefore, trigeminal nerve pain can result from an overworked and fatigued jaw muscle, an inflamed jaw joint, a cracked or decayed tooth, or a simple gum infection.
Therefore, most of the suffering due to trigeminal nerve pain occurs as a result of problems that can be readily diagnosed and treated effectively by trained practitioners. Most importantly, these problems are common, familiar, and helpable when evaluated and treated by trained practitioners.
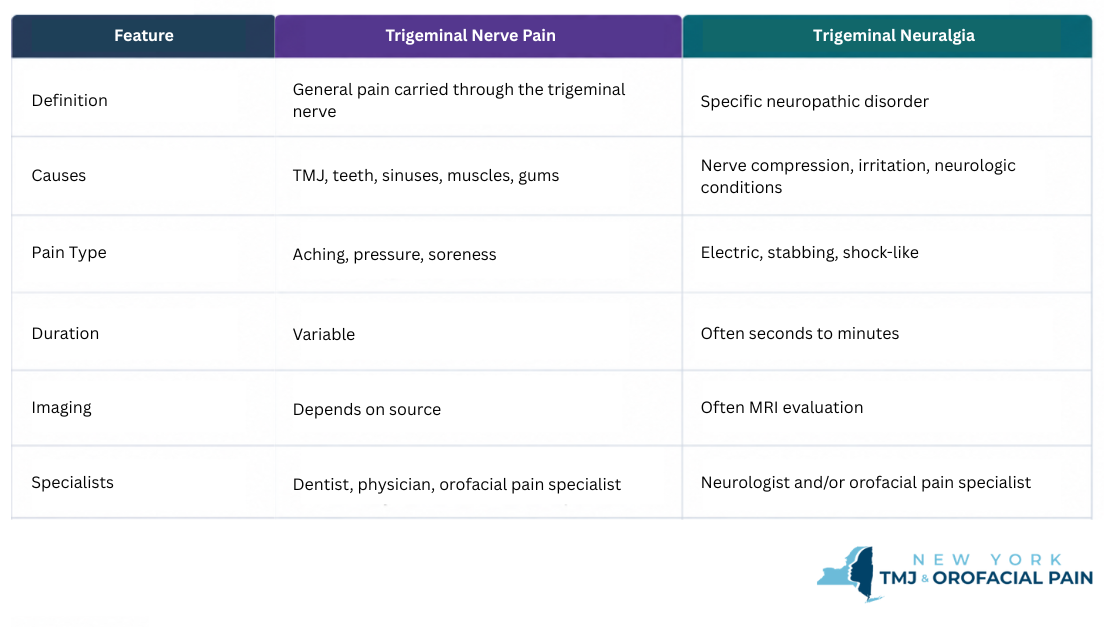
What is the difference between trigeminal nerve pain and trigeminal neuralgia?
Trigeminal nerve pain is a broad term describing pain signals carried by the trigeminal nerve from the teeth, jaw muscles, TMJ, gums, sinuses, or facial tissues. Trigeminal neuralgia is a specific neuropathic pain disorder that usually causes sudden, severe, electric-shock-like facial pain.
Because both conditions involve the trigeminal nerve, trigeminal neuralgia can sometimes feel like tooth pain, jaw pain, or a TMJ problem. A careful history, examination, and sometimes imaging are needed to determine the true source of pain.
For patients who have undergone multiple dental, medical, or TMJ evaluations without a clear diagnosis, an orofacial pain evaluation can help identify whether symptoms are more consistent with trigeminal neuralgia, TMJ-related pain, dental pain, or another facial pain condition.
What Is Trigeminal Neuralgia?
Trigeminal neuralgia (TN) is a distressingly painful, sometimes debilitating, and often chronic neuropathic pain condition. Trigeminal neuralgia typically affects the middle or the lower part of the face on one side. As it is classified as a type of neuropathic pain, it is mostly caused by damage or disease to the nervous system’s sensory component.
The pain of trigeminal neuralgia can be felt in the face, teeth, gums, lips, and mouth region and tends to be sporadic, electrical or shock-like, and is often combined with a burning sensation. Patients frequently describe spark like electrical sensations during an attack.
Approximately 60% of all patients often diagnosed with trigeminal neuralgia start seeking care from a dentist because they are experiencing bad toothache pain. Yet, evaluations and x-rays taken in the dental office usually do not reveal the real problem. Despite a lack of findings, treatment such as root canals is often initiated treatment such as root canals are often started as a way to relieve a patient’s suffering. Unfortunately, these efforts fail to solve the problem.
The pain of TN has some unique features. The pain may be experienced in the midst of an otherwise pain-free day appearing without provocation, or it can be triggered by speaking, drinking, eating, brushing the teeth, or causal contact of the face around the lips and nose.
Unlike most other facial pain problems, trigeminal neuralgia pain can be manageable or miserable all within several minutes of a day. People with trigeminal neuralgia often report being pain-free and then incapacitated for seconds or minutes until the pain vanishes or subsides to a low level. Trigeminal neuralgia attacks can become more frequent and intense over time.
Why Trigeminal Neuralgia Can Feel Like a TMJ Problem
Patients with trigeminal neuralgia often describe severe limitation of jaw motion during an attack of TN due to spasm of the jaw muscles, which are directly under the influence of the trigeminal nerve. For this reason, TN has also been called tic douloureux, with the ‘tic’ describing the severe facial muscle spasm. Due to the restricted jaw motion described by patients, this problem can be misdiagnosed as TMJ.
As mentioned, the diagnosis of trigeminal neuralgia is most commonly made based on the unique character of the symptoms the patient describes. The examination of the face and the painful areas is often unremarkable unless there are distinct trigger zones that, when touched, fires the pain.
Brain imaging MRIs or MRAs may be ordered in order to detect whether there is an underlying medical condition such as MS, a tumor, or blood vessel compression of the nerve causing the TN pain.
Finally, trauma to the face, jaw, or teeth can injure the trigeminal nerve and lead to what is called traumatic TN.
Common Treatment Options for Trigeminal Neuralgia
Once a tentative diagnosis has been made, medications are usually the first-line treatments. Multiple medications may be used together and changed over time if effectiveness is lost. These medications are designed to reduce the nerve sparking and excitation, but unfortunately do not cure trigeminal neuralgia.
Other treatments may be beneficial as well, including nerve blocks and, at times, BOTOX® injections. Topical medications, both inside the mouth and on the face, have also shown some promise in controlling daily symptoms.
When these treatment efforts fall short despite collaboration with multiple experts in the field, neurosurgery is the next step to be explored.
Other Types of Trigeminal Neuropathic Pain
There is an “atypical” form of TN called TN2. Instead of short episodes of disabling pain, patients with TN2 experience continuous pain with burning and aching features. Although the pain of TN2 is less intense than TN, its constant presence is often thought to be more disruptive to a patient’s life as there is no downtime.
Continuous neuropathic pain problems also require medications to ease suffering. However, because continuous nerve pain can lead to muscle tension and splinting, TN2 symptoms can be confused with a TMJ problem.
In summary, pain within the trigeminal system is a primary reason that patients seek care in my practice. Fortunately, once a diagnosis has been made, many of these problems are common, familiar, and helpable.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
Not Sure If Your Pain Is TMJ, Tooth Pain, or Trigeminal Neuralgia?
Facial pain can be difficult to diagnose because the trigeminal nerve carries pain signals from many facial structures.
If your pain has not been clearly diagnosed, an orofacial pain evaluation can help determine the most likely source.
New York TMJ & Orofacial Pain evaluates patients with facial pain, jaw pain, tooth-like pain, TMJ symptoms, and nerve-related pain at office locations in Manhattan, Long Island, Westchester, and Northern New Jersey.
Donald R. Tanenbaum, DDS, MPH, is Co-Founder of New York TMJ & Orofacial Pain and a board-certified specialist in Orofacial Pain. Together with his colleagues, he helps evaluate and manage patients with temporomandibular disorders (TMD), complex facial pain, neuropathic pain conditions, headaches, and sleep-related disorders. New York TMJ & Orofacial Pain is a referral resource for medical and dental professionals seeking specialized care for patients with challenging orofacial pain and jaw disorders. The practice has office locations in Manhattan, Long Island, Westchester, and Northern New Jersey.
Frequently Asked Questions Trigeminal Nerve Pain vs. Trigeminal Neuralgia
Is trigeminal nerve pain the same as trigeminal neuralgia? No. Trigeminal nerve pain is a broad description of pain carried by the trigeminal nerve. Trigeminal neuralgia is a specific neuropathic pain disorder.
Can trigeminal neuralgia feel like TMJ?
Yes. Many patients initially believe they have TMJ pain because trigeminal neuralgia can affect the jaw area.
Can trigeminal neuralgia feel like a toothache?
Yes. Trigeminal neuralgia frequently mimics dental pain and may lead patients to seek dental treatment before receiving an accurate diagnosis.
What does trigeminal neuralgia pain feel like?
Patients often describe sudden electric-shock-like, stabbing, or burning facial pain.
Who should I see for facial pain that might be trigeminal neuralgia?
A neurologist and/or an orofacial pain specialist may be involved depending on the symptoms and diagnosis.
Can TMJ problems irritate the trigeminal nerve?
TMJ disorders can generate pain signals carried by the trigeminal nerve, but this does not necessarily mean a patient has trigeminal neuralgia.
When should someone in the NYC area see an orofacial pain specialist?
Patients should seek evaluation when facial pain, jaw pain, tooth-like pain, or nerve pain persists despite prior dental or medical treatment, or when the diagnosis remains unclear.
At times we see a patient with TMJ symptoms, but something just doesn’t seem right. Instead of the usual history of most of my patients, which can include tooth grinding and clenching, neck tension, excessive worry and anxiety, and jaw clicking, this patient is experiencing jaw and facial pain for what appears to be no good reason. Jaw motion and function are normal, but pain persists on a daily basis.
A number of these patients have medical histories that include long-term gastrointestinal distress (IBS, Reflux, Gerd, and/or Crohn’s Disease), unexplained skin rashes, and joint pains throughout the body. As a result of these symptoms, they’ve consulted multiple medical specialists who have determined that an underlying autoimmune condition is causing spontaneous inflammatory pain and low pain thresholds.
An Intimate Relationship Between the Immune System & Persistent Pain
There appears to be an intimate relationship between the immune system and the part of the nervous system involved in the experience of persistent pain. Every day your immune system talks to your nervous system (and therefore, your brain) and helps to maintain comfort or sets off alarms if something is wrong such as a virus, infection, dehydration, low blood sugar, etc.
At times, however, people can experience pain because the immune system has told the nervous system that something is wrong – when nothing really is wrong.
It’s become obvious that face and jaw pain can be caused by autoimmune problems. Therefore, the likelihood that traditional treatments, such as jaw exercises, injections, and oral appliances, will fall short. Muscles and joints may only be the site of your symptoms but not the direct cause.
We treat many patients with autoimmune problems. We depend on the strong relationships we have with our physician colleagues in rheumatology and immunology to help these patients with a great deal of success.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
Over the last 10 to 15 years, there has been a great deal of research looking at the relationship between sleep and pain. As a result of these studies, it is now very clear that pain thresholds are significantly impacted by both the quality and quantity of your sleep.
If the quality and quantity of your sleep are compromised, your pain thresholds drop, which can lead to situations where pain is experienced in your muscles and joints on a daily basis. This is in spite of the fact that no clear evidence of joint or muscle injury exists. Rather, your pain is experienced as a result of normal activity and accentuated when muscles or joints are overworked.
Many people who are seen in our office describe pain in their muscles and joints as a result of normal eating and even talking. This points to the possibility that the nerve endings in their jaw muscles and joints are operating at a low threshold and, therefore, they experience pain almost all the time. This is called allodynia: when normal stimulation generates pain. In addition, excessive jaw use from teeth clenching and grinding produces even higher levels of pain beyond what is normally expected. Poor sleep can lead to all of these TMJ symptoms.
If you have insomnia (the inability to get to sleep or stay asleep), your pain thresholds can drop significantly. You may experience morning headaches and/or an assortment of body pain symptoms during the course of almost every day.
Sleep quality is also impacted if you have airway difficulties. If you’ve been diagnosed with upper airway resistance or respiratory effort-related arousal, your pain symptoms are commonly in your head and neck region. Headaches and temporomandibular problems are very common in people with airway challenges. Many patients who grind and clench their teeth (bruxism) have been shown to have airway problems, and some are diagnosed with obstructive sleep apnea.
There is an association (not an absolute relationship) between fragmented sleep and the occurrence of grinding and clenching activity. If you wake up with sore or tight jaw muscles, it is likely a result of bruxism activity.
We will ask you many questions about your sleep history during the evaluation process. Most sleep problems can be helped in my office. If your problem is more complex, we will consult with a sleep professional to help you get on the road to feeling better.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
On a routine basis, we are asked whether or not stress could be responsible for the onset of a patient’s facial pain. The answer to this question is a resounding “Yes!”
But there are 3 things to understand in order to appreciate how this occurs and why it is so common:
Aside from toothache pain, the most common reason that people experience facial pain is muscle strain.
Muscle strain that lingers gives rise to symptoms such as pain and or restrictions in movement.
The muscle pain and malfunction that we see occurs as a result of subtle changes in the chemical environment of a muscle, and this is most often influenced by a stressed brain.
This is What Happens
When you are under stress for a long period of time, or when your emotional world is characterized by anger, sadness, loneliness, loss of control, worry, and anxiety (to name just a few), the brain becomes understandably upset. As a result, the brain is unable to provide exquisite control over blood flow, muscle tension, and nerve discharge, that are essential for muscle comfort. Loss of this control leads to an accumulation of irritating chemicals in your muscles, like lactic acid and others, that leads to pain and muscle tightening.
In the presence of this irritating chemical environment the nerves that run through your muscles fire excessively, and pain along with muscle tightening results. In essence, a brain under emotional siege sets the stage for muscles to falter.
2 More Things to Understand
With ongoing emotional turmoil, it is likely that both the quality and quantity of your sleep will suffer. As a consequence, your muscles are more likely to ache, with the experience of muscle tension headaches, facial pain, and jaw pain being common.
A brain under siege commonly leads to learned behaviors and tendencies such as tooth clenching, raised shoulders, furrowed brows, crossed arms, and shallow breathing patterns that can predispose to more pain and a continuous cycle of suffering.
Thoughts alone can, over time, give rise to facial pain symptoms. Through our experience, insight, and treatment strategies, it is likely that we can ease your pain and set you on the path to recovery.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
The concept of referred pain has been around for over 50 years. It is used to describe the phenomenon of pain experienced at a site nearby or even at a distance from the pain’s origin.
It’s likely you have heard that one of the most common symptoms of a heart attack is pain in the left arm or shoulder. This is a pattern of referred pain. Fortunately, this pattern of symptom description is now well recognized, allowing medical professionals to deliver care to the right place – the heart – instead of the wrong place – the arm!
In the face, mouth, and jaw, the experience of referred pain is common. Routinely we see patients with tooth pain, gum pain, jaw pain, and ear pain when in fact, the origin of the pain symptom is coming from elsewhere. Unfortunately, patients choose the doctor they visit based on the symptom location, and this can produce a great deal of confusion and, at times, treatment directed at the wrong place.
At first, the examining doctor has no choice but to look at the site of the pain complaint, but if no findings are uncovered, the thinking of the doctor must change and focus on possible sources of referral. When the focus is not changed, treatment is delivered without success leading to patient frustration.
Though the neurologic basis behind referred pain is complicated, there are several things to understand.
Referred pain typically does not cross the midline. If the problem area generating the pain is on the right side of the body, the pain that is experienced is also on the right.
It is most common for referred pain to move upwards in the body. That is, pain is typically referred from the neck and shoulder to the face and jaw, not vice versa.
Not surprisingly, if the location of the pain experienced is treated and the origin is neglected, the pain will continue.
Though muscles are involved in the majority of referred pain problems that we see, blood vessels and nerves can also be involved in pain referral leading to more comprehensive evaluations.
As you can imagine, referred pain is often a difficult and challenging problem for patients and physicians. As a result, our evaluation is always focused on the sources of possible referral, not just on where the symptoms are focused.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
In my practice, we see 4 distinct categories of facial pain problems.
Muscle and joint pain problems
Nerve pain problems
Tension Headache and Migraines
Chronic widespread pain (formerly called fibromyalgia)
It would seem that these problems could affect anyone, but in fact, the vast majority of patients that walk through the door of our practice are women. Believe it or not, somewhere between 78% and 82% of all the patients we see are female.
In the past, this dominance of women was attributed to social and cultural factors that prompted women to seek care more frequently than their male counterparts. Though women do seek care more frequently than men for a number of medical problems, research in pain biology has provided evidence that there are unique factors that are likely driving this huge statistical difference, particularly in the face and jaw.
The Estrogen Connection
One big biologic difference between men and women relates to the hormone estrogen. Studies have shown that variable levels of estrogen not only have the ability to impact the effectiveness of the body’s endorphins (our natural pain fighters) but can also increase inflammation associated with the Temporomandibular Joints (TMJ). During times of persistent stress, compromised sleep, and monthly menstrual cycles, estrogen levels fluctuate sufficiently to prompt pain to emerge in unexpected ways not commonly seen in men.
As estrogen is known to compromise the strength and adaptive capacity of ligaments throughout the body, the TM joints are a common location for problems to surface. As a result, the supportive jaw ligaments in women are likely to become more readily compromised when subject to the forces of normal function and certainly to excessive functions like gum chewing, nail and cuticle biting, and clenching or grinding of the teeth. As a result, symptoms of jaw clicking, popping, and locking are more likely to occur, persist and escalate in women when compared to men.
Also, when considering the biologic differences between men and women, it is worth mentioning that the jaw muscles of men have greater endurance than similar muscles in women. This likely occurs as the jaw muscles of women receive less blood flow (and therefore less oxygen and nutrients) than the same muscles in men, making them more susceptible to tiring more easily during both normal and excessive jaw use.
As a result, as oxygen levels in muscle tissue drops, the chemical makeup of the muscle changes with lactic acid and other irritating substances accumulating over time. These chemical changes lead to muscle soreness initially and then muscle weakness and susceptibility to spasms as time passes. These factors, therefore, may be responsible for the predisposition women have to developing facial and jaw pain and problems associated with jaw motion.
In attempting to understand why women have much more profound pain experienced in the Temporomandibular joints, the impact estrogen potentially has in increasing the intensity and persistence of inflammation cannot be overlooked. Specific estrogen receptors in the TM joints of women must, therefore, not be overlooked when trying to understand the predisposition of women to these often debilitating problems.
Within this category of diverse sufferers, we again see a female dominance. Though the reasons for the onset of these very different pain problems in all individuals are not fully understood, there is evidence that each of these pain problems, to some degree, is connected to lowered nerve firing thresholds. Research has, in fact, suggested that these lowered nerve-firing thresholds that lead to pain are the result of an individual’s genetic makeup (an individual’s phenotype) and or due to changes in an individual’s genetic makeup due to environmental influences. These are called epigenetic changes. One or both of these factors are often responsible for changes in the way the brain interprets sensory signals received from all parts of the body.
When normal sensory signals received from bodily tissues are interpreted as noxious, an individual becomes predisposed to pain problems. As over 60% of all sensory information reaching the brain comes from the oral and facial region, women who more commonly have these genetic or epigenetic profiles will suffer to a greater extent whether the initiating factors were traumatic events of all degrees, environmental challenges, sleep compromises and/or life stressors of all types.
As the medical community begins to understand this biologic predisposition to facial pain and jaw-related problems, women who come to my office are not categorized as complainers who can’t handle life’s tensions and challenges. Rather, we understand the complexity of these problems and don’t blame the person. We focus on putting the best treatment strategies together that will confront not only the pain-prompting biology but also the person who is in trouble.
With the success that we have achieved over the years, you should be optimistic that there are answers to your problems.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.











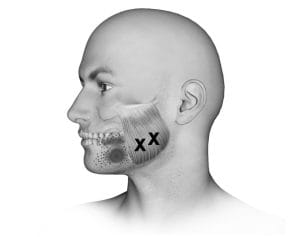
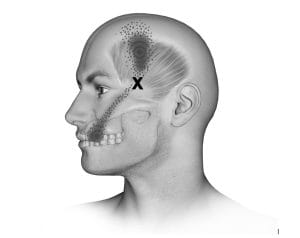





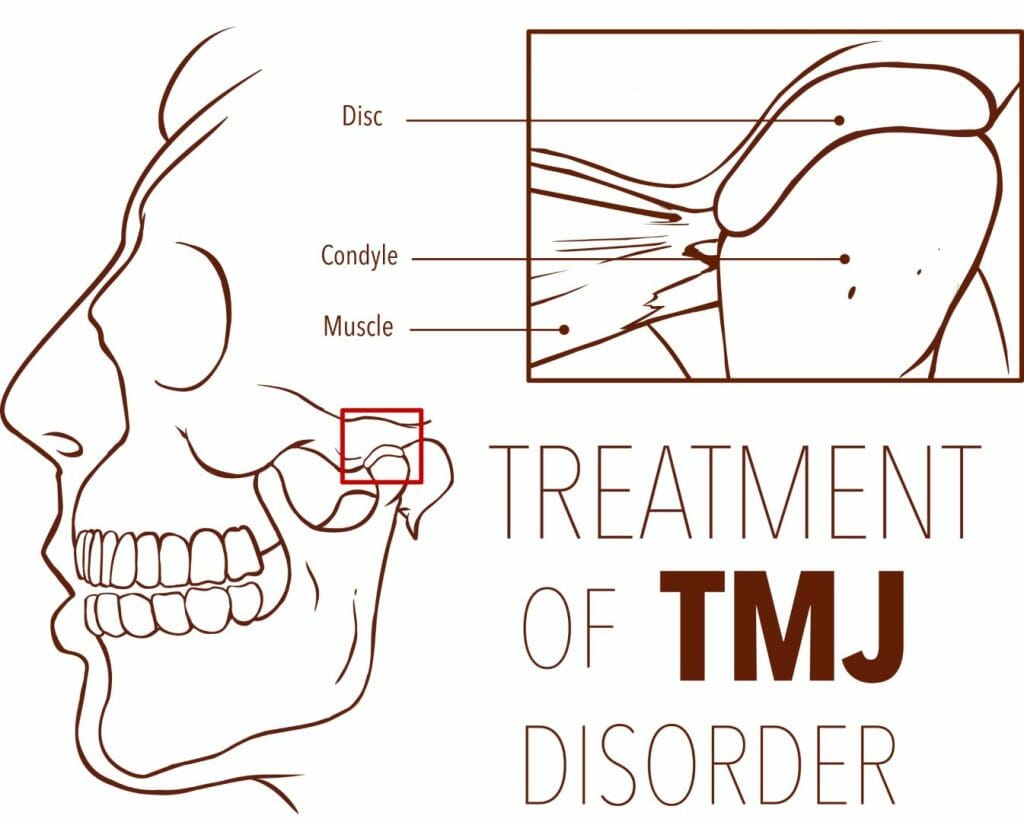 The best treatments for TMJ always start with an accurate diagnosis. Not every pain in the face and jaw is due to a TMJ disorder. In fact, the broad term Orofacial Pain is now used to describe any discomfort or pain in the mouth, face, and neck region, including the jaw joint (temporomandibular joint or TMJ), muscles, teeth, and nerves.
The best treatments for TMJ always start with an accurate diagnosis. Not every pain in the face and jaw is due to a TMJ disorder. In fact, the broad term Orofacial Pain is now used to describe any discomfort or pain in the mouth, face, and neck region, including the jaw joint (temporomandibular joint or TMJ), muscles, teeth, and nerves.



 There’s another possible reason you have TMJ pain. Many people rely on medications such as Adderall, Ritalin, Concerta®, and Vyvanse® to enhance their brain focus. While they’re effective, they can also stimulate your internal fight-or-flight system, which in turn can lead to jaw over-use behaviors, which in turn can cause jaw problems.
There’s another possible reason you have TMJ pain. Many people rely on medications such as Adderall, Ritalin, Concerta®, and Vyvanse® to enhance their brain focus. While they’re effective, they can also stimulate your internal fight-or-flight system, which in turn can lead to jaw over-use behaviors, which in turn can cause jaw problems.