
There’s a good chance you landed here because you’ve been suffering from an unexplained toothache, a persistent sinus pain that won’t leave you alone, or an annoying earache that makes you wince every time you chew for a long time. These symptoms have likely sent you on multiple visits to healthcare professionals, each one leaving you with more questions than answers.
But what if the source of your pain is not where you’re feeling it?
Your puzzling array of symptoms just may be due to problems with your temporomandibular joints (TMJs) and associated muscles. Your TMJs and jaw muscles play a fundamental role in the basic movements of your jaw—talking, chewing, yawning, and even expressing emotions. When this joint and its corresponding muscles and ligaments become strained, unstable, and or overworked, the resulting condition is known as temporomandibular disorder or TMD.
When a TMD problem is not considered as a source of pain in teeth, the ear and/or sinus, for example, the result can be ongoing evaluations and treatments that address the location of the pain symptoms but not the origin. When the location of the pain complaint is not the true origin, the term referred pain is commonly used.
Referred Pain & Its Relationship To TMD Problems
Referred pain is pain perceived at a location other than the origin of the painful stimulus. It is the result of a network of interconnecting sensory nerves that are persistently over-excited. For example, when there is an injury or pathology at one site in the network, it is possible that when the signal is interpreted in the brain, mistakes are made as to the true origin of the problem. As a result, pain is often experienced at a distance from the true origin. (E.g., pain from a heart problem is experienced in the shoulder or jaw)
So, how does this relate to the structures of the jaw?
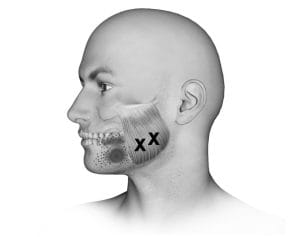
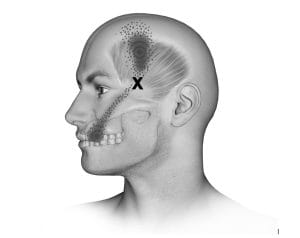
When your jaw muscles (masseters and temporalis) are persistently overworked, they become sore, extremely sensitive, and knotted. These areas are known as trigger points. When activated, trigger points can send pain signals to places far from their origins, resulting in referred pain. Jaw overuse behaviors such as clenching your teeth during the day, biting your nails, chewing your pens, etc., can lead to the formation and activation of these trigger points, leading to referred pain in areas such as your teeth, ears, or sinuses.
Orofacial Pain Specialists Understand What You’re Going Through
As part of an Orofacial Pain practice, my colleagues and I are well-versed in the nuances of this disorder. For many of our patients, merely validating their pain and helping them understand the concept of referred pain gets them moving in the right direction on the road to recovery.
If you’re nodding your head right now, thinking, “That’s me!” I encourage you to seek the care of an Orofacial Pain specialist. Your treatment plan might include education, awareness strategies to reduce jaw overuse behaviors and fatiguing postures, oral appliances, exercises, and/or relaxation techniques to address daily worries and stress. In addition, physical therapy can also be helpful, along with muscle injections, to break up the trigger points that are driving your pain.
How To Get Help Now
If you live in the NYC metro area and are ready to uncover the root of your Orofacial Pain, we are here to guide you. Take the first decisive step by scheduling a consultation at one of our convenient offices in Manhattan, White Plains, New Jersey and on Long Island. Together, we’ll get to the bottom of what’s causing your suffering and get you on the road to recovery.
If you’re outside the NYC metro area, the American Board of Orofacial Pain website has a national directory of Orofacial Pain specialists.
Find out more about TMJ pain:
TMJ Headaches & Migraines
Pain & The Brain







2 comments on “The Secret Behind Unexplained Toothaches & Facial Pain”
I am UK based so cannot seek treatment with you but your blog especially the article on thr PDL has made so much sense to me. I fell on my face knocking the jaw snd UL1and 2 . Pulpitis ensued but pain was worsened with each of the three root canals. Dentist suspected ann invisible crack as the pain was atypical. No evidence of a crack and tbe canals now only show minor apical lesion and healing. Now taking amytriptiline following oral surgeon consult and the worst of the facial. pain is diminished after 5 weeks. But by about 5 ish the teeth involvex or gums have a lot of pain and occasional swelling if they are touched/ moved. This does respond to codeine. The likelihood that this is an ongoing issue of the PDL makes great sense. I had a heavy fall on that area and then three invasive treatments in rapid succession.
Samantha,
So sorry to hear of your troubles. Best of luck and I hope you feel better soon.
Dr. Tanenbaum