TMJ surgery has received some negative press over the years. You may have read horror stories on the Internet about TMJ surgery gone bad. The reality is countless patients would still be living with acute jaw pain and limited jaw motion if they had not had surgery as an option.
I’ve spent the past 40 years focused almost exclusively on treating patients with TMJ and facial pain problems. I’m often asked how I determine when TMJ surgery is needed.
Non-Surgical Treatments Are Always Tried Before Surgery Is Ever Considered
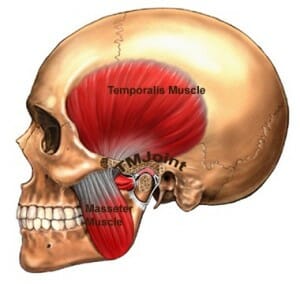
It’s important to understand that TM joint problems are orthopedic problems – just like tennis elbow or a rotator cuff injury, for example. Sometimes, tissue injury in the TM joints is severe and involves compromised ligaments, stubborn inflammation, displaced cartilage, and/or arthritic and erosive problems affecting the bones.
If your TM joint pain is due to inflammation, and after we’ve tried all non-evasive therapies, our one last non-surgical effort is steroid injections into the “hot” joint.
The success of steroid treatment depends upon how long you’ve experienced pain, the origin of your problem, the condition of your underlying bone, ligaments and cartilage, and your ability to avoid new injury to the joint. If progress is made after the first injection, a second is usually administered in about three months.
However, when no relief is experienced after the first injection, the steroid method is put aside.
When Steroid Injections Don’t Work – The Next Option Is Arthrocentesis
If steroid injections are unsuccessful, the next option is usually arthrocentesis. Arthrocentesis is a procedure whereby your injured TM joint is, in essence, washed-out to remove the irritating chemicals that accumulate when you have tissue injury.
In addition, your injured TM joints may not move easily due to sticky adhesions. So, the second goal of arthrocentesis is to break down these adhesions, which allows your joint to move more easily. When movement is easier, so are your prospects of healing. (Arthrocentesis is usually performed under local anesthetic and light sedation.)
As with steroid injections, supportive therapies are put in place afterward such as oral appliances, home treatments and exercises, dietary caution, oral medications, and physical therapy.
When Arthrocentesis Doesn’t Work, Is TMJ Surgery Next?
Like any orthopedic problem, there are times when all non-surgical treatments fail.
The procedure of choice in this instance is arthroscopic surgery. Arthroscopic surgery allows your doctor to visualize the damage in your TM joint and effectively remove any adhesions, smooth any irregular bone, and inject steroids right into areas that are inflamed. We often take tissue biopsies at the same time.
When performed by experienced hands, arthroscopic surgery is extremely effective in starting the process of natural healing, which for most patients, results in profound pain reduction and increased ease of jaw motion. Although usually performed under general anesthesia, arthroscopic surgery is an outpatient procedure.
(Home exercises and/or physical therapy are always required after arthroscopic surgery.)
When All Else Fails
If the MRI and CT scans reveal extreme tissue damage, extensive bone erosions, and/or degenerative arthritis, then we may need to surgically open the joint. Opening the joint enables extensive repairs to be made, but it requires special surgical skills and experience. Like all the procedures outlined in this article, long-term rehabilitation is put in place and is required.
A full regimen of non-surgical care must always be attempted before TMJ surgery is ever considered. TMJ surgery can repair injured tissues, relieve (or even eliminate) pain, and improve your jaw function. But it should be always considered as the last resort.
The Takeaway: If you do need surgery, ongoing collaboration between your dentist, a board-certified orofacial pain specialist, your surgeon, and your physical therapist must exist in order for you to heal and experience long-lasting results.
To find a board-certified orofacial pain specialist in your area, visit The American Academy of Orofacial Pain and look for a doctor with Diplomate status.