During this time of year, it is common for my practice to see many patients who experience symptoms of TMJ from scuba diving or snorkeling. In fact, it has been reported that between 15%-20% of the people who scuba dive or snorkel have some level of jaw problem.
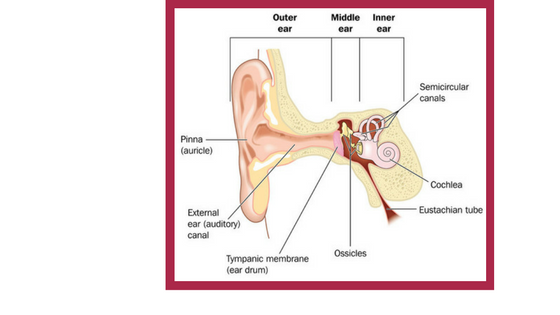
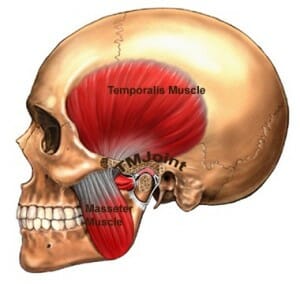
To find out why you first must understand the temporomandibular joints (TM’s) and how they function. Your TMJs are the hinges that connect your upper jaw to your lower jaw. They enable you to open and close your mouth in a smooth, unrestricted way. When functioning properly, your TMJ’s allow you to chew, talk, and yawn in comfort.
But because the TMJ’s are moved by muscles and stabilized by ligaments, any problem with those muscles and ligaments will have a negative effect on the function of your jaw and your comfort. People whose TMJs are overworked may experience pain, limited jaw opening, joint noises, and sometimes even a change in the way their teeth come together. The symptoms are very similar to an overworked knee.
TMJ From Scuba Diving Or Snorkeling Is Very Common. Here’s Why:
Whether you scuba dive or snorkel, your lower jaw must come forward to secure your breathing mouthpiece in place. It’s a very awkward position and when held for a long period of time, it fatigues your muscles and strains your ligaments. The result can be soreness, pain, and limited jaw function.
New divers are at the greatest risk for TMJ from scuba diving or snorkeling. The novice has a tendency to fiercely grip down on the mouthpiece for fear of it slipping out of place. This forceful clenching can set jaw problems into motion. And a poorly fitted mouthpiece is often a culprit, too.
Prevention & Treatment of TMJ from Scuba Diving Or Snorkeling
As an orofacial pain specialist, I have some advice for you if you are a new or inexperienced diver here’s some advice: try to maintain a loose grip on your mouthpiece and always make sure it fits properly. (If you suspect it doesn’t…don’t use it! Trade it in ASAP.) If mild symptoms start to occur, don’t dive for a day or two. Try anti-inflammatory medications such as Advil or Aleve, if tolerated. And ice packs on painful areas for seven minutes several times a day can also help.
If experiencing severe symptoms and just a day or two off from diving doesn’t improve your condition, you should see a dentist who focuses on temporomandibular disorder. TMJ is the result of tired, tight, injured or sore muscles, inflamed tendons, or compromised ligaments, bone and cartilage. As a result, TMJ treatment is similar to what is offered by an orthopedist when managing a knee problem.
Here are some of the ways we treat patients with TMJ from scuba diving or snorkeling at my practice:
- Limiting the overuse of the jaw by dietary restrictions
- Identifying strategies to reduce daytime habits that may prevent healing such as clenching, nail and cuticle biting, gum chewing
- Medications to reduce inflammation and muscle tension
- Supporting the injured joints or muscles with an oral appliance
- Home jaw exercises and self-massage of jaw muscles
- Physical therapy if needed
- Trigger point injections for pain and tension in the jaw muscles
It’s best to avoid TMJ from scuba diving or snorkeling by taking precautions such as loosening the grip on your mouthpiece and making sure it fits properly. Stop your diving activities if symptoms start and seek care to assure healing. The vast majority of our patients do heal and happily resume their diving activities after several months.
Live or work in New York City or on Long Island? You can schedule a consultation with me here or call 212-265-0110.