One of the most common questions about dentistry that people ask on Google is this: “Why are my teeth so sensitive?”.
Unfortunately, there’s no simple answer to this question. There could be any number of reasons why your teeth are sensitive, some of which may surprise you. In the following article, I list 8 reasons your teeth are sensitive and a brief explanation of each. Does one apply to you?
8 Reasons Your Teeth Are Sensitive
1. Your Toothpaste Is Too Abrasive
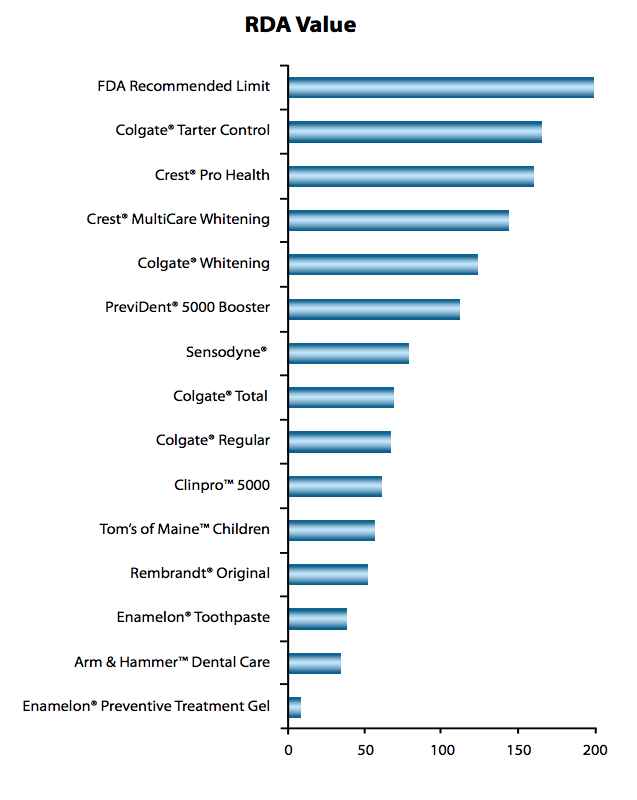
In order for toothpaste manufacturers to gain approval from the FDA they must measure and report the abrasiveness of their products. However, they are not required to report the information to consumers. To help you find out how your favorite toothpaste stacks up, refer to the chart below. Your teeth are sensitive perhaps because of the toothpaste you’ve been using.
2. You’ve Been Using Whitening Toothpaste
Whitening toothpastes often contain chemicals that help to remove surface stains and therefore, make your teeth much whiter. However, these chemicals can damage the surface of your teeth. Several whitening toothpastes have received the American Dental Associations’ (ADA) Seal of Acceptance. However, it is recommended that you consult your dentist before using whitening toothpaste to avoid damage. So, if you’ve been brushing with whitening toothpaste and your teeth are sensitive, whitening toothpaste may be the culprit.
3. There’s Too Much Acid In Your Diet
Citric acid, such as what’s found in lemons, oranges, and grapefruits, can be very damaging to your tooth enamel. It’s not hard to understand how too much citric acid could cause erosion of your teeth enamel and therefore, sensitive teeth.
On the other hand, most people don’t realize that many popular beverages, many of which don’t seem to be acidic, are very acidic. My colleague, New York dentist Michael Sinkin, warns: “…many vitamin waters, energy drinks, and sports drinks are highly acidic and if consumed in large quantities can cause your teeth’s structure to break down.”
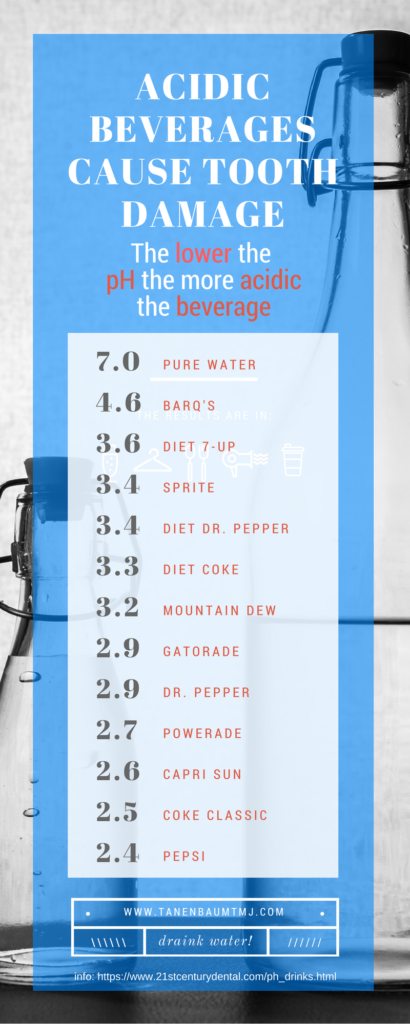
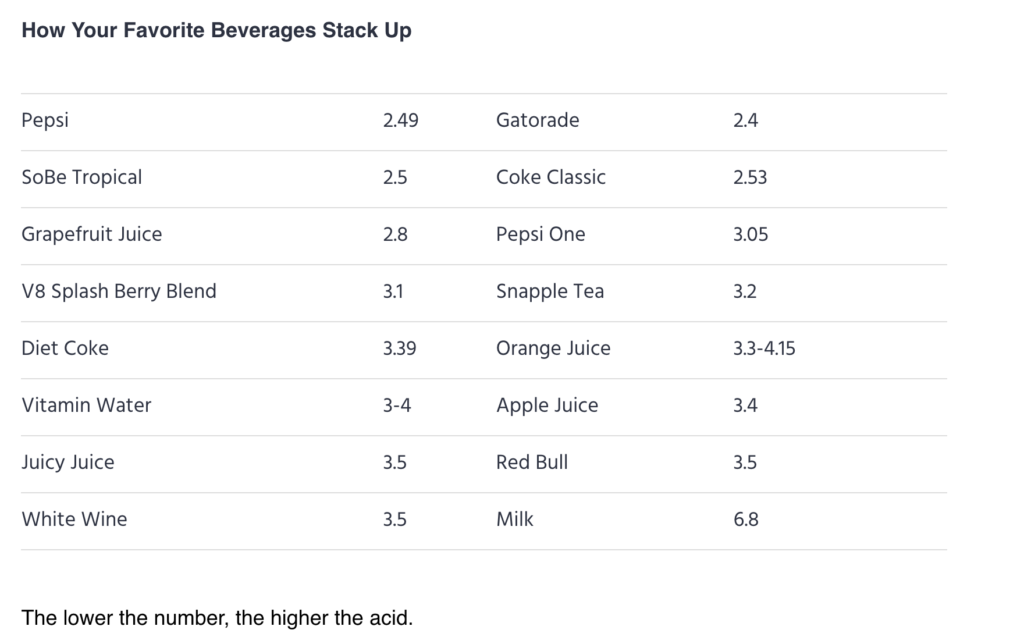
So, how can you find out if your favorite beverage contains enough acid to be the reason your teeth are sensitive? Check the pH! pH is the measure of acidity on a scale of 1-14. The lower the number the higher the acidity; tooth enamel begins to dissolve at pH 5.3.
The chart below shows the pH of some popular beverages. If you’ve been gulping Gatorade at the gym or if you slug down a Red Bull every afternoon to fight tiredness, those beverages may be the cause of your sensitive teeth.
Source:
http://michaelsinkindds.com/is-your-favorite-beverage-eroding-your-tooth-enamel/
4. You’re A Swisher!
The next time you drink a soda, juice, or a glass of wine, take note if you swish it around in your mouth before you swallow. Many people swish their beverages without realizing it, which can create a loss of tooth enamel and sensitize the teeth’s dentin and cementin. Wine connoisseurs in particular, who swish in order to better experience the nuances of vintages, are at especially at risk. It’s OK to swish a little, but try keeping it to a minimum.
5. Your Teeth Need A Cleaning
Even people with the means to go to their dentist two or three times a year often avoid it because of dental fear. You can floss and brush twice a day, every day, but it’s nearly impossible to remove all the tartar and plaque that will build up on your teeth naturally. When plaque builds up around and under your gums, it will cause inflammation, and therefore, sensitive teeth.
If you haven’t been to the dentist for a while you could be surprised to discover that most practices now are hyper-aware of how anxious some patients can be, even when they come in just for a simple cleaning. Dental fear is nothing to be ashamed of, so discuss it with your dentist and get those teeth cleaned!
6. You Breathe Through Your Mouth
Chronic sinusitis from allergies or a deviated septum can cause you to continually breathe through your mouth instead of through your nose. An article in RDH, The National Magazine For Dental Hygiene Professionals, states: “Mouth breathing affects the pH of the entire body… meaning the saliva.”
In other words, breathing through your mouth over a long period of time can actually make your saliva more acidic and could be the reason your teeth are sensitive. The best advice is to see an ENT (an Ear, Nose and Throat doctor) as soon as possible.
7. Your Jaw Muscles Are Being Overused
I’ve been treating patients who have tooth and jaw problems that stem from overworked jaw muscles for over 35 years. If you hold tension in your face and keep your teeth clenched together during the day, your jaw muscles are being overworked. Overworked jaw muscles can cause headaches, facial pain, persistent toothache, and sensitive teeth. Try to relax your jaw, especially when you’re working at your desk. For more help, read Problems of the Jaw.
8. You Grind Your Teeth While You’re Sleeping
Nighttime teeth grinding, also called Bruxism, is a common phenomenon that causes your jaw muscles to over-contract. In fact, some people grind their teeth so ferociously that they actually sprain their jaw ligaments, which is why their teeth are sensitive.
My practice is full of people who suffer from bruxism and just want to feel better. Our first step is to figure out what’s causing the grinding. Only once the underlying reasons are discovered can we put in place a treatment plan to eliminate the grinding and therefore, its damaging efforts.
Did you figure out why your teeth are sensitive? Whatever the cause, keep in mind that your sensitive teeth are a sign that something is going on. Don’t ignore it.
(Note: If the cause of your tooth sensitivity is related to overuse behaviors or nighttime teeth grinding and you live in the NYC metro area, please feel free to (212)-265-0110 for a consultation. If you’re outside my area, you can go to www.aaop.org and find a Diplomate in your area.)
Read More:
Tooth Whitening/Bleaching: Treatment Considerations for Dentists and Their Patients