
A case study in nonodontogenic dental pain and the diagnostic value of pain journaling
When dental pain persists despite negative clinical and radiographic findings, the answer often lies beyond the tooth itself. This case illustrates how thorough assessment and pain journaling can reveal nonodontogenic sources, transforming both patient outcomes and diagnostic confidence.
When it’s everything but the tooth
“Jason,” a 49-year-old entrepreneur, felt his life was derailed by persistent pain that he was certain originated from tooth number 30. It was a tumultuous time with business to close and year-end tasks to complete. This relentless pain was making everything worse.
He was so convinced the tooth was the culprit that he had consulted his dentist and endodontist nearly two years prior, receiving multiple root canal treatments between teeth numbers 30 and 31. But his pain continued to worsen, and his endodontist didn’t believe that a third root canal would help. Desperate for answers, Jason found our practice.
“It’s a dull, annoying throb,” he exclaimed, “and it’s driving me crazy.” Jason relied on multiple tablets of acetaminophen and ibuprofen when the pain occurred “randomly” each week. When it escalated to an excruciating level, he turned to hydrocodone for relief. These episodes happened several times per month and radiated from his lower right teeth and gums into his jaw and right ear.
When examination reveals nonodontogenic sources
Upon careful examination, it became clear that neither intraoral examination nor radiographic imaging revealed a source of pain. There was no percussion or palpation tenderness within the oral soft tissue or teeth, no signs of infection or swelling. Yet, Jason’s pain was undeniably real and debilitating.
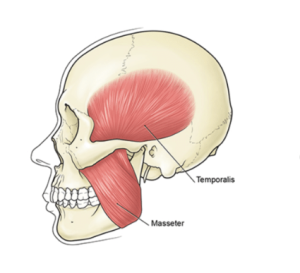
The most significant findings told a different story entirely. Jason had an overbuilt and tender masseter muscle on the right side, coupled with a notable malocclusion. His teeth contacted predominantly on the right posterior dentition, specifically teeth numbers 30 and 31, with only light contact on tooth number 18 on the opposite side.
Jason had lived with this asymmetric bite for several years. “My orthodontist could never resolve this,” he would say. Furthermore, Jason had never been informed about the importance of keeping his teeth apart throughout the day. He was unaware that even light tooth contact at rest could result in persistent masticatory muscle contraction.
His pain pattern offered additional clues. What Jason described as “random” episodes actually followed identifiable triggers, though this only became apparent through systematic documentation. The radiation beyond typical dental patterns, extending to his jaw and ear, combined with his escalating medication reliance despite multiple dental treatments, suggested we were dealing with nonodontogenic dental pain.
Although the clinical presentation was not as revealing as expected, the story was there.
Using pain journaling to solve the puzzle
Given Jason’s pain history and growing medication dependence, we initiated trigger point therapy using 2% lidocaine into the right masseter muscle that same day. This was a treatment that would be both diagnostic and therapeutic in nature.
His treatment was followed by a thorough explanation of behavior avoidance techniques and pain journaling. Our goal was to determine whether these seemingly random episodes could reveal a pattern.
It wasn’t until consistent documentation of his symptoms paired with better isolation of his pain, following treatment, did he realize something significant: Treatment of the right masseter muscle resulted in a reduction of pain that was originally perceived to be in his lower right tooth!
The pain was no longer random but had identifiable triggers.
When patterns emerge, everything changes
By the second appointment, Jason was able to identify the frequency of his pain and noted that it seemed to follow stressful periods or alcohol consumption. Through our guidance, he became aware of clenching behaviors that predominantly impacted teeth numbers 30 and 31 due to his malocclusion.
His transformation was remarkable. Within one month, his pain medication reliance decreased, and he felt less stress and greater confidence knowing he could better predict his symptoms. The trigger point therapy paired with pain journaling provided Jason with the confidence he needed to set positive recovery in motion and regain autonomy over his health.
Understanding what was really happening
Jason was clearly experiencing severe myofascial pain referral to the lower right teeth and gums. The source of his pain was the masseter muscle, which had been overworked, fatigued, and received minimal attention for nearly two years due to parafunctional activity beyond his awareness, combined with a previous misdiagnosis.
Could the dentist be blamed when the patient seemed adamant that it was coming from his tooth? This level of pain severity is not commonly seen with myofascial pain referral, but it can occur depending on chronicity and individual risk factors. The alcohol may have contributed to pain exacerbation due to consequential skeletal muscle tightening and decreased hydration.
Without a complete symptom history and thorough physical assessment, this type of nonodontogenic dental pain can be tricky for dentists to diagnose.
Jason continued to improve with several treatments of targeted trigger point therapy. We have plans to discuss treatment options with his dentist to address remaining sleep parafunction and malocclusion.
The power of pain journaling for complex cases
One of my favorite things about Jason’s story is that he learned how valuable pain journaling can be, alongside self-awareness, in maximizing treatment outcomes. Pain journaling is especially valuable in nonodontogenic dental pain cases when symptoms don’t align with clinical and radiographic presentation.
To start, I often recommend documenting:
- When the pain occurred (date, time of day)
- Which actions, if any, preceded it (chewing, workouts, sleep)
- Where it occurred (right or left side, one location or several)
- Quality of pain (dull, achy, sharp, electrical, burning)
- Pain duration (hours vs seconds)
- What, if anything, successfully decreased the pain
This information can be presented at initial visits and follow-up appointments to enhance patient assessments. The appointments we offer at New York TMJ & Orofacial Pain permit the valuable time needed to review pain journals and guide patients accordingly. Documentation like this contributes to diagnostic accuracy and provides patients with confidence in both their provider and themselves.
For complex cases where dental findings don’t match patient symptoms, early collaboration between dental and orofacial pain specialists can prevent prolonged patient suffering and inappropriate treatments. We diagnose and treat many different types of pain conditions throughout the head and neck. Documentation like this can save time during assessments and better organize the history of pain. Jason’s case reminds us that sometimes the most persistent dental pain has nothing to do with the tooth at all.
About Dr. Werfel

Dr. Aimee Werfel is a licensed general dentist with specialized Orofacial Pain training through Rutgers School of Dental Medicine. She practices at our Manhattan location and instructs residents at Weill Cornell–NY Presbyterian. An active member of the American Academy of Orofacial Pain and American Headache Society, her expertise and educational commitment reflect her dedication to advancing orofacial pain management.
If You Practice in the NYC Metro Area:
If you are located in the NYC metropolitan area, New York TMJ & Orofacial Pain has four locations fully staffed with board-certified orofacial pain specialists who are ready to help your patients.
Learn About Our Practice
Learn About Our Treatments
Learn More About Trigger Point Therapy for Orofacial Pain
For further clinical context on nonodontogenic dental pain and related conditions: Nonodontogenic toothache: diagnostic challenges and clinical considerations.
Frequently Asked Questions About Nonodontogenic Dental Pain
- What is nonodontogenic dental pain?
Nonodontogenic dental pain is persistent tooth pain that originates from sources other than the tooth itself, such as overworked muscles like the masseter. Patients often feel certain the pain comes from a specific tooth, but dental examination and imaging reveal no dental pathology. - How can dental professionals identify when dental pain might have non-dental sources?
Key indicators include: no percussion or palpation tenderness in teeth, no radiographic evidence of pathology, no signs of infection or swelling, pain that radiates beyond typical dental patterns (to jaw and ear), and symptoms that persist despite appropriate dental treatment. - What role does pain journaling play in diagnosis?
Pain journaling helps identify patterns in seemingly “random” pain episodes. Patients document when pain occurred, what preceded it, where it occurred, pain quality, duration, and what decreased it. This systematic documentation often reveals triggers like stress or specific behaviors. - Why might dental professionals miss these non-dental pain sources?
Without a complete symptom history and thorough physical assessment, this type of pain can be tricky to diagnose. Patients are often adamant that pain comes from a tooth, making it challenging to look beyond dental sources. - What triggers commonly cause nonodontogenic dental pain?
Based on this case, common triggers include stressful periods, alcohol consumption, and unconscious clenching behaviors. Malocclusion and unawareness of daytime tooth contact can contribute to persistent masticatory muscle contraction. - How effective is trigger point therapy for this condition?
Trigger point therapy can be both diagnostic and therapeutic. In this case, treating the masseter muscle with lidocaine resulted in reduction of pain originally perceived as tooth pain, confirming the muscle as the actual source. - When should dental professionals refer to orofacial pain specialists?
Early collaboration is recommended for complex cases where dental findings don’t match patient symptoms. This prevents prolonged patient suffering, inappropriate treatments, and escalating medication dependence. - What can patients expect from nonodontogenic dental pain treatment?
With proper diagnosis and treatment, patients can experience decreased medication reliance, better symptom prediction and control, and regained autonomy over their health. Treatment often includes trigger point therapy, behavior modification, and addressing contributing factors like malocclusion.
