
Case Study: Hypermobility and Ehlers-Danlos Syndrome
For a broader clinical overview, see our discussion of hypermobility and TMJ disorder
Clinical perspective
TMJ disorders in hypermobile patients often present with excessive range of motion, joint instability, and chronic muscular compensation, rather than the restricted patterns more commonly seen in typical TMD cases.
Patient history
“Melissa” was 26 when she first came to the practice. She had been diagnosed with hypermobile Ehlers-Danlos Syndrome two years earlier, after a long history of what she described as being “someone who always got hurt for no reason.”
She reported sprains that took months to heal, shoulder subluxations during routine activities, and back pain that began in high school and never fully resolved.
Her jaw had been a problem for most of her adult life, but she had not connected it to her connective tissue diagnosis until her EDS specialist mentioned that TMJ involvement is common in hypermobile patients.
Clinical findings
Melissa presented with bilateral preauricular pain, prominent joint clicking on both sides, and an opening of 52 millimeters, which she had always assumed was normal.
Examination of the masticatory system revealed:
- Diffuse tenderness of the masseter and temporalis muscles
- Muscle pain that was not focal, but consistent with chronic overuse
- Joint sounds suggestive of disc displacement and instability
The overall pattern was not one of restriction, but of excessive mobility with compensatory muscular activity.
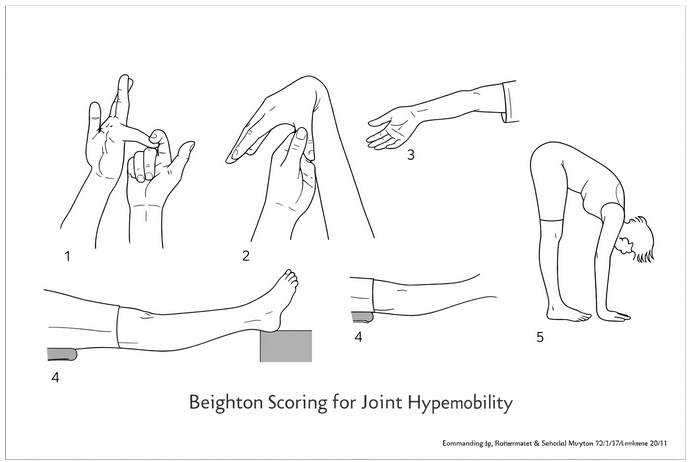
Findings were also consistent with generalized joint hypermobility, typically assessed using tools such as the Beighton scoring system.
Diagnosis considerations
In patients such as Melissa, the diagnostic framework shifts from identifying isolated joint pathology to understanding the interaction between structural instability and muscular compensation.
Her presentation was consistent with:
- TMJ instability in the setting of connective tissue laxity
- Chronic myofascial pain secondary to prolonged muscular guarding
- A history of incomplete recovery following repeated micro and macro trauma
The underlying collagen disorder provides the context in which these findings develop and persist.
Treatment approach: managing, not curing
The treatment framework for hypermobility-related TMJ disorders is not fundamentally different from standard orofacial pain management, but the goals are recalibrated.
The focus is on stability, symptom management, and prevention of further deterioration, rather than resolution of the underlying condition.
Education and validation are essential. Patients with hypermobile Ehlers-Danlos Syndrome often have a long history of symptoms that have been misunderstood or minimized. Understanding the biological basis of their condition is itself therapeutic.
Key components of management include:
- Reduction of daytime parafunctional behaviors to minimize repetitive micro-loading
- Use of an oral appliance during sleep to reduce nocturnal joint loading
- Dietary modification to avoid excessive mechanical stress
- Behavioral strategies to limit extreme jaw opening, including wide yawning
Physical therapy plays a central role, particularly when directed toward muscular stabilization. The goal is to strengthen the masticatory and cervical musculature so that it can provide support in the absence of normal ligament integrity.
Trigger point injections may be used to address persistent myofascial pain associated with chronic muscular overuse.
Prolotherapy in hypermobility
In this patient population, prolotherapy warrants specific attention.
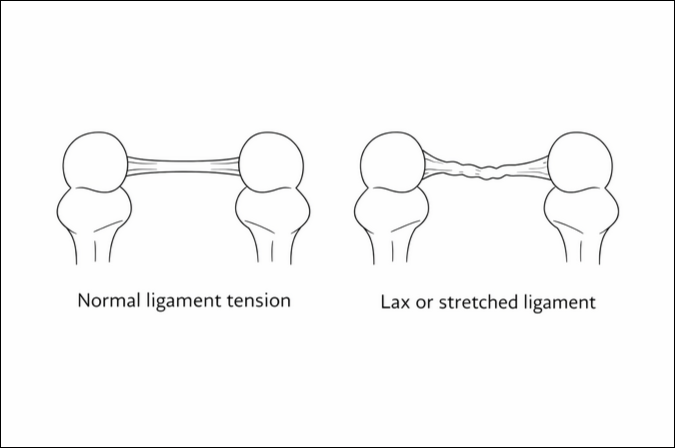
Prolotherapy involves the injection of a dextrose solution into ligamentous attachment sites and the joint capsule, with the goal of stimulating a controlled inflammatory response.
This process promotes new collagen deposition, which can improve ligament tensile strength and reduce joint laxity over time.
For patients in whom joint instability is a primary driver of symptoms, prolotherapy is not simply an adjunctive therapy. It can be a central component of the treatment strategy, particularly when conservative measures alone are insufficient.
Clinical perspective
When Melissa was told that the goal of treatment was to help her feel better and function more reliably, rather than to correct the underlying connective tissue disorder, she responded that it was the most honest explanation she had received about her condition.
That perspective reflects an important aspect of managing hypermobility-related TMJ disorders.
A clear understanding of biological limitations, combined with a structured approach to stabilization and symptom management, allows for meaningful improvement even in the absence of a definitive cure.
Referral considerations
Patients with TMJ disorders in the setting of hypermobility or Ehlers-Danlos Syndrome often require a more specialized approach to diagnosis and management.
When instability, excessive range of motion, or persistent symptoms despite standard care are present, referral may be appropriate.
For our colleagues in the New York City metropolitan area
If your practice is located in the New York City metropolitan area, New York TMJ & Orofacial Pain has four locations staffed by board-certified orofacial pain specialists. We provide evidence-based, multidisciplinary care and collaborate closely with referring providers to achieve optimal patient outcomes.
Related articles by our doctors
Three Pathways to TMD: Mind-Body, Trauma, and Medical Causes
Two TMD Case Studies – Connective Tissue Disorders
Sex, Gender, and Pain: A Review of Recent Clinical and Experimental Findings
Related study
Image Citations
The Temporomandibular Joint – Musculo-Skeletal Key
Surgical Approaches to the Temporomandibular Joint Esmaeelinejad, Mohammad & Sohrabi, Maryam. (2018).
The Ehlers-Danlos Syndrome: Steinmann, Beat & Royce, Paul & Superti-Furga, Andrea. (2002).
