If you see patients with temporomandibular disorders (TMD) in your practice, as I have over the last 40 years in the New York metropolitan region, you already know that the overwhelming majority are women. The ratio holds across cultures, age groups, and healthcare settings. Between 77% and 82% of patients seeking care are female. That consistency is not coincidence. It is biology.
Understanding why women are more vulnerable matters. It directly influences how we interpret patient history, how we set expectations for recovery, and which treatments we prioritize.
Case Study: “Jordan”
Jordan was 22 years old when she first came to our office. She was a college senior. Her jaw had been tightening for approximately four months. Some mornings she woke with an ache that took an hour to resolve. Eating had become something she considered before doing, and she had begun avoiding foods that required significant chewing.
Her history reflected a familiar pattern.
Jordan’s mother had been diagnosed with breast cancer eight months earlier. Attending college near home, Jordan had reorganized her life around caregiving responsibilities while managing her coursework. She was not sleeping well. She described lying awake worrying and waking unrested. Caffeine became essential.
She had bitten her nails since childhood but had never experienced jaw symptoms. Under increased stress, the habit intensified. Not only nails, but cuticles as well. She was rarely aware of the behavior. Her partner had noticed grinding sounds at night, which she initially dismissed.
Symptoms eventually emerged and persisted, prompting evaluation.
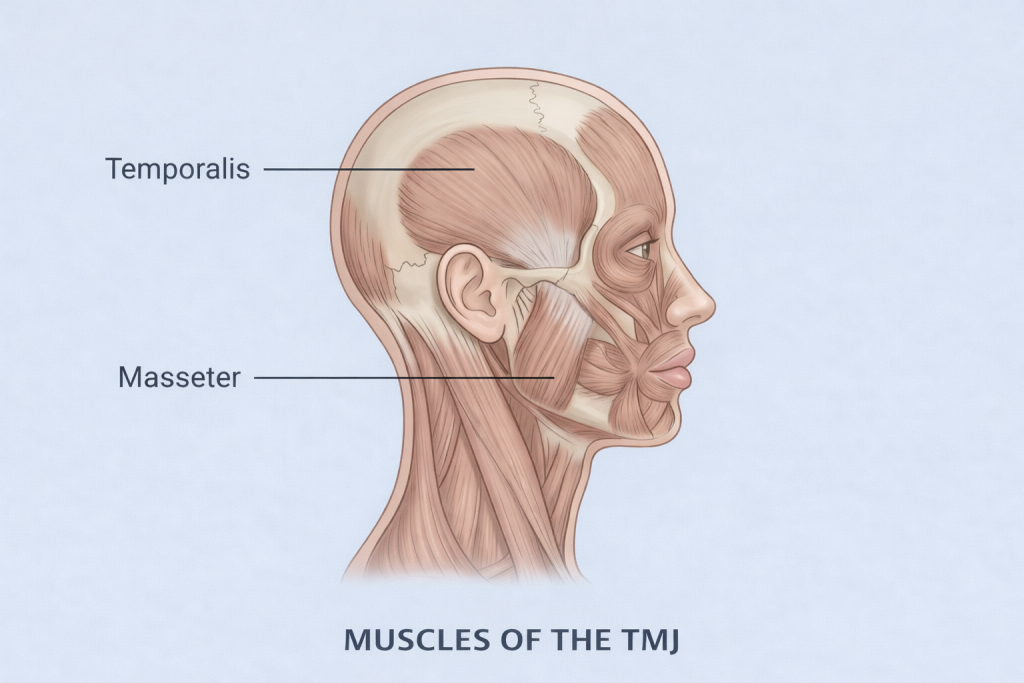
Following examination, her masseter and temporalis muscles were tender bilaterally. Jaw opening was restricted, and pain increased with forced opening. A subtle click was present in the left joint, which was also tender to palpation. Her masseter muscles were well developed and prominent on tooth contact.
Nothing about this presentation was unusual. What required explanation was why a patient of her age, without a single traumatic event or known medical condition, developed this level of dysfunction.
The joint itself is different
The temporomandibular joint in women contains an abundance of estrogen receptors, both ER alpha and ER beta. When estrogen binds to these receptors, elastin production increases, promoting ligamentous laxity. At the same time, collagen synthesis becomes less structurally organized compared to men. The result is greater joint laxity and reduced load-bearing capacity.
For Jordan, this meant that nail biting, which required the lower jaw to thrust forward against resistance, was placing mechanical stress on joint structures that were inherently less stable. Behaviors that may be tolerated in other patients were, in her case, contributing to dysfunction in a joint already at a structural disadvantage.
Her sleep bruxism compounded this effect. The nightly clenching and grinding observed by her partner reflected sustained nervous system activation. Instead of restorative recovery during sleep, her jaw muscles and joints were subjected to repeated loading. Micro-injury accumulated faster than it could resolve.
The pain system is different
Beyond structural considerations, women process pain differently at a neurobiological level.
Androgens, including testosterone, enhance pain inhibitory mechanisms through descending modulation pathways associated with the neurotransmitter GABA. Women, with lower androgen levels, have less biologic support within this system.
Excessive jaw activity can trigger inflammatory mediators that activate pain-amplifying pathways while simultaneously reducing inhibitory control. The result is a self-reinforcing cycle of sensitization.
The same mechanical overload that produces temporary soreness in one patient may lead to persistent pain in another. This reflects differences in the neurochemical environment, not differences in resilience.
For Jordan, prolonged stress contributed to sustained sympathetic activation. This state depletes neurotransmitters, including GABA, that support inhibitory pain control.
She was not fragile. She was physiologically disadvantaged in ways that are measurable and clinically relevant.
What this means for treatment
Biologic sex does not represent a separate disease pathway, but it significantly influences how the three most common origins of TMD, mind-body stress, physical trauma, and underlying medical conditions, present clinically.
For Jordan, treatment addressed each contributing factor.
The nail biting required behavioral awareness and interruption strategies. Sleep bruxism warranted an oral appliance and evaluation of sleep quality. The emotional burden of her mother’s illness required more than general stress reduction.
She required targeted nervous system support. Breathing techniques helped regulate autonomic function. She was referred to a therapist experienced in caregiver stress and health-related anxiety.
Equally important was education. When she understood that her joint structure and pain processing were influenced by biology, her experience became clearer and more manageable.
Female patients whose symptoms persist despite appropriate physical treatment are not treatment failures. Their biology creates a lower threshold for sensitization and a higher barrier to recovery through physical intervention alone.
Clinical perspective
Understanding why TMJ disorders are more common in women changes clinical decision making.
Recognizing the influence of joint biology, pain modulation, and stress physiology leads to more effective care. These patients often require multidisciplinary management as a central component of treatment.
Jordan improved over four months of coordinated care. Jaw opening normalized. Morning discomfort decreased. Her external stressors remained, but her nervous system no longer expressed that burden through persistent jaw pain.
The underlying cause informs the treatment approach.
For our colleagues in the NYC Metropolitan area
If your practice is located in the New York City metropolitan area, New York TMJ & Orofacial Pain has four locations staffed by board-certified orofacial pain specialists.
We provide evidence-based, multidisciplinary care and collaborate closely with referring providers to achieve optimal patient outcomes.
To contact one of our offices click here.
Learn more
Learn About Our Practice
https://www.nytmj.com/for-referring-doctors/
Learn About Our Treatments
https://www.nytmj.com/tmj-treatments-we-provide-nyc/
Related articles & studies
Advances in Temporomandibular Disorders: Insights for Dental Professionals
Three Pathways to TMD: Mind-Body, Trauma, and Medical Causes
Sex, Gender, and Pain: A Review of Recent Clinical and Experimental Findings
