
Managing the Aftermath of Self-Treatment
Case Overview
“Jessica”, a 26-year-old woman, presented to our practice with persistent bilateral masseter pain and a newly developed anterior open bite following self-directed care.
Her symptoms began after a prolonged dental appointment two years earlier. To manage her discomfort on her own, Jessica began using an over-the-counter (OTC) nightguard purchased at a pharmacy and intermittently took muscle relaxants prescribed by different providers. Over time, her pain persisted and her bite gradually changed.
Finally, as her symptoms continued and her bite felt increasingly unstable, Jessica sought an orthodontic consultation, believing that her teeth now needed realignment. Fortunately, the orthodontist recognized that the underlying issue was not orthodontic in nature and referred her to our practice, New York TMJ & Orofacial Pain. Shortly afterward, she was evaluated in our office.
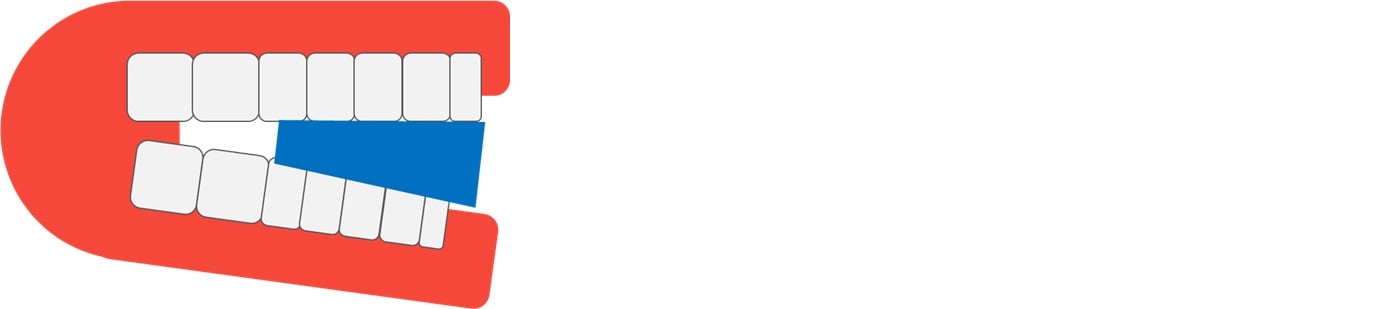
On examination, palpation of the masseter muscles reproduced her familiar pain. She demonstrated normal mandibular range of motion and no TMJ noises. Notably, occlusal contact occurred only on the posterior molars (#18, 19, and 31), with a clear anterior open bite. Imaging showed no evidence of TMJ degeneration.
The pattern was consistent with super-eruption of posterior teeth caused by long-term use of a partial-coverage OTC appliance.


Note that only the posterior teeth are in contact.
Over-the-Counter Mouthguards
Over-the-counter mouthguards have some advantages, namely cost and availability. But there are also disadvantages, some of the more commonly cited being:
- Discomfort. They have a less precise fit and greater bulk than well-designed custom appliances.
- Lack of rigidity. People are more likely to “chew” on the soft materials used in the fabrication of stock mouthguards.
- Inability to accurately control jaw position during the night. This is of particular importance for people suffering from TMJ disc displacement disorders.
The other major disadvantage of over-the-counter mouthguards is their propensity to cause bite change with long-term use. This occurs because they rarely cover all of the posterior teeth, leading to super-eruption of the uncovered teeth. This is likely what caused Jessica’s bite change:



Treatment and Management
Jessica’s treatment required addressing both occlusal correction and pain reduction.
The first step was discontinuation of the OTC appliance. With time and observation, partial occlusal recovery was expected as the super-erupted teeth equilibrated. Behavioral counseling focused on minimizing daytime clenching and habitual “bite checking.”
Pain management included targeted botulinum toxin injections to the masseter muscles to reduce nocturnal activity while the occlusion stabilized. Appliance therapy was deferred until her bite could be reassessed.
At her three-month follow-up, Jessica reported near-complete resolution of pain and a partial improvement in tooth contact (her second premolars were now touching). Ongoing quarterly monitoring was planned, with the goal of completing orthodontic correction and then fabricating a custom, full-coverage nightguard once her occlusion stabilized.
Clinical Takeaways for Referring Providers
OTC nightguards remain a common source of iatrogenic occlusal change. Patients like Jessica often use them without realizing the risk of worsening both pain and bite alignment. Asking specifically about self-directed appliance use can be critical when evaluating patients with unexplained open bites or persistent muscle pain.
Early referral to an orofacial pain specialist allows for proper diagnosis, management of muscle-based pain, and eventual design of a safe, full-coverage custom appliance.
Conclusion
When patients self-treat with OTC nightguards, the result can be more than persistent discomfort—it can be a lasting change in occlusion. Recognizing these cases early and providing targeted, evidence-based management prevents long-term functional and esthetic complications.
(For a review of published cases documenting occlusal derangement following night-guard use, see Bereznicki et al.)
Learn About Our Practice
Expert Q&A
- How can I identify occlusal changes caused by OTC nightguards?
Patients often report new difficulty achieving anterior contact, or “bite feels off,” following appliance use. Clinical signs include anterior open bite, posterior supraeruption, or uneven occlusal contacts. Partial-coverage appliances are a strong indicator of risk. - What history details help confirm self-treatment behavior?
Ask specifically whether the patient purchased a mouthguard at a pharmacy or online and how long they have used it. Many patients omit this detail unless prompted, assuming OTC devices are harmless. - When should OTC appliance use be stopped immediately?
Discontinue use as soon as there is evidence of bite alteration, worsening pain, or uneven occlusal contact. Continuing wear can make these changes more pronounced and harder to reverse. - Can open bites from partial-coverage appliances self-correct?
Mild cases may improve partially once the appliance is discontinued, as the occlusion re-equilibrates. However, moderate to severe anterior open bites often require orthodontic or restorative intervention after stabilization. - What role does botulinum toxin play in managing masseter myalgia?
Botulinum toxin reduces hyperactivity in the masseter muscles, minimizing clenching intensity and facilitating recovery while other conservative measures take effect. It can be especially useful during the occlusal stabilization phase. - How long should occlusal adaptation be monitored after discontinuation?
Typically, re-evaluation at 8–12 weeks is appropriate. Some improvement can be seen within a few months, but full stabilization may take longer depending on the extent of supraeruption and the patient’s parafunctional habits. - What defines a safe, custom occlusal design for bruxism and TMJ pain?
A properly designed appliance provides full-arch coverage, uniform occlusal contact, smooth guidance, and freedom from posterior interferences. Design and follow-up should always be tailored to the patient’s diagnosis and functional patterns. - How can we best educate patients to avoid self-directed appliance use?
Reinforce that not all nightguards are the same. Explain that OTC devices can unintentionally shift the bite and worsen pain, whereas custom appliances are precision-fitted and supervised. Positioning this as part of preventive oral health care helps patients understand the value of professional oversight.
More articles by our staff:
