Clinical insight
In patients with joint hypermobility or Ehlers-Danlos Syndrome, TMJ disorders are often driven by structural instability rather than restriction, requiring a different diagnostic and management approach.
Every patient who walks through the door of an orofacial pain practice carries a story about how their jaw problem began. In most cases, that story fits one of three familiar frameworks.
There was a physical event such as a fall, a prolonged dental procedure, a car accident, or a bite on something that resisted.
Or the problem developed gradually under the weight of the mind-body axis, where chronic stress is expressed as clenching and bruxism, and the jaw muscles carry what the nervous system cannot put down.
Or an underlying medical condition created the biological environment in which jaw problems were more likely to occur.
In practice, most patients present with some combination of all three. The trauma lands harder on a system already compromised by stress. Bruxism does more damage when the connective tissue holding the joint together is constitutionally fragile. Inflammation does not resolve when the underlying medical contributor remains active.
It is that third category, underlying medical conditions, that this discussion addresses, and specifically one that has been appearing in clinical practice with increasing frequency: generalized joint hypermobility and its most recognized expression, Ehlers-Danlos Syndrome, and their role in the development of TMJ disorders.
In a specialty orofacial pain practice serving the New York City metropolitan area, this pattern is being seen with increasing regularity.
The role of connective tissue
Ehlers-Danlos Syndrome is a group of heritable connective tissue disorders characterized by abnormally elastic and fragile collagen. The hypermobile subtype is the most common and the one most frequently encountered in clinical practice.
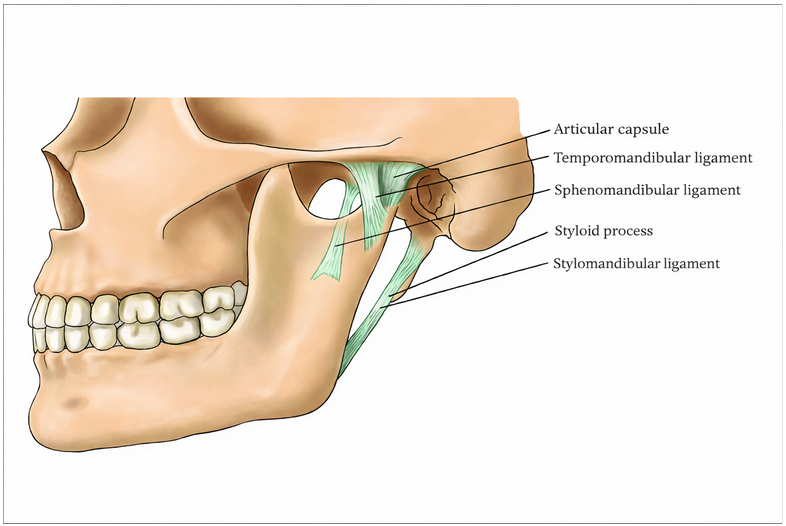
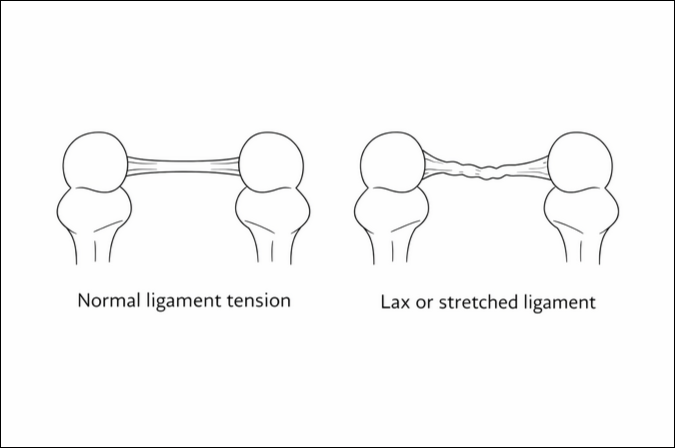
In these patients, the collagen that forms ligaments, joint capsules, tendons, and fascial layers does not provide normal structural integrity. Joints are lax. Ligaments stretch beyond their intended range and do not fully return. The mechanical boundaries that normally contain joint movement and protect articular surfaces from excessive load are less reliable.
In the temporomandibular joint, this has significant implications. The disc, ligaments, and capsular tissues all depend on collagen integrity to maintain their function. When that integrity is reduced, the disc is less well restrained, the joint becomes susceptible to micro-instability, and the inflammatory response to repeated low-level trauma is more difficult to resolve.
The tissue that is expected to recover between functional demands cannot fully return to its prior state because the structural environment is inherently compromised.
Hypermobility is a risk factor, not a diagnosis
It is important to state clearly that generalized hypermobility does not inevitably lead to a TMJ disorder. Many hypermobile individuals remain asymptomatic.
Hypermobility creates a predisposition, lowering the threshold at which the joint can be destabilized. Clinical symptoms emerge when additional contributing factors are present.
Several factors are particularly relevant:
- Hormonal influences, particularly in female patients, contribute to increased ligamentous laxity and pain sensitivity
- Daytime parafunctional behaviors, including clenching and posturing, introduce repetitive microtrauma
- Sleep bruxism increases joint loading during the period when recovery should occur
- Macrotrauma, such as injury or dental procedures, may not heal back to baseline in structurally compromised tissue
When these factors converge, the likelihood of persistent joint instability and chronic symptoms increases substantially.
Why symptoms develop
In hypermobile patients, the temporomandibular joint often functions with reduced structural restraint. As a result, the surrounding musculature must compensate to maintain stability.
Over time, this leads to:
- Chronic muscular overuse
- Myofascial pain and fatigue
- Joint noise associated with disc displacement
- Inflammatory changes that are slow to resolve
A key clinical distinction is that instability, rather than restriction, is often the dominant issue in this population.
TMJ disorders in hypermobile patients
A recognizable pattern has become more common in clinical practice. Patients, often in their twenties or thirties, present with jaw pain, joint noise, and a range of motion that exceeds what is typically expected.
Where many TMD patients present with restricted opening, these individuals often demonstrate opening measurements of 50 millimeters or greater, reflecting underlying joint laxity.
Clinical examination frequently reveals:
- Diffuse muscle tenderness consistent with chronic overuse
- Prominent joint sounds, reflecting disc displacement and instability
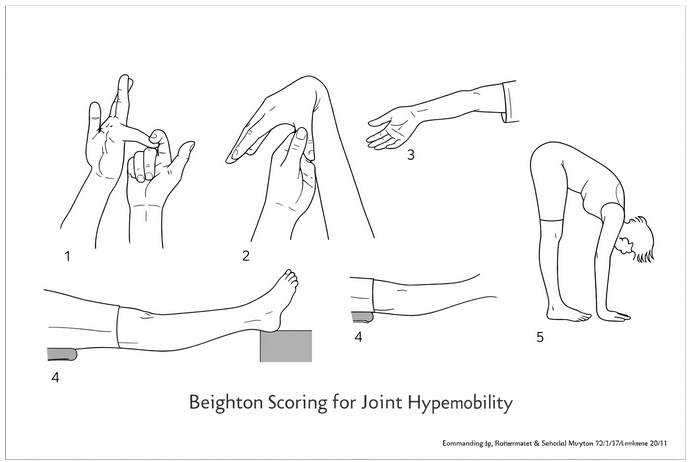
- Generalized joint hypermobility, often supported by Beighton scoring
- Associated connective tissue findings, including skin hyperextensibility
Many of these patients have received a relatively recent diagnosis of hypermobile Ehlers-Danlos Syndrome, often after years of unexplained symptoms affecting multiple joints.
Referral Considerations
Patients with persistent TMJ symptoms in the setting of joint hypermobility or suspected connective tissue disorders often require a more specialized diagnostic and management approach.
When joint instability, excessive range of motion, or lack of response to standard care is present, further evaluation may be appropriate.
Case application
See our accompanying case study on TMJ disorders in hypermobility and Ehlers-Danlos Syndrome.
For our colleagues in the New York City metropolitan area
If your practice is located in the New York City metropolitan area, New York TMJ & Orofacial Pain has four locations staffed by board-certified orofacial pain specialists. We provide evidence-based, multidisciplinary care and collaborate closely with referring providers to achieve optimal patient outcomes.
Related articles by our doctors
Advances in Temporomandibular Disorders: Insights for Dental Professionals
Three Pathways to TMD: Mind-Body, Trauma, and Medical Causes
Understanding TMJ Subluxation Treatment: A Closer Look at “Open-Lock”
Related study
Temporomandibular disorders among Ehlers-Danlos syndromes: a narrative
Image Citations
Surgical Approaches to the Temporomandibular Joint Esmaeelinejad, Mohammad & Sohrabi, Maryam. (2018).
The Ehlers-Danlos Syndrome: Steinmann, Beat & Royce, Paul & Superti-Furga, Andrea. (2002).
