A Mechanism-Based Approach to Persistent Post-Surgical Facial Pain
Persistent pain following technically successful structural oral or facial surgery presents a clinically challenging scenario. When the surgical site has healed, imaging is unremarkable, and inflammation is controlled, yet pain persists, mechanism-based evaluation becomes essential.
In these cases, clinicians must differentiate structural pathology from neuropathic or nociplastic pain. “Nociplastic” is the term put forth by the International Association for the Study of Pain to describe pain arising from altered nociception without clear evidence of tissue damage or peripheral nerve injury.
The Case – “Debbie”
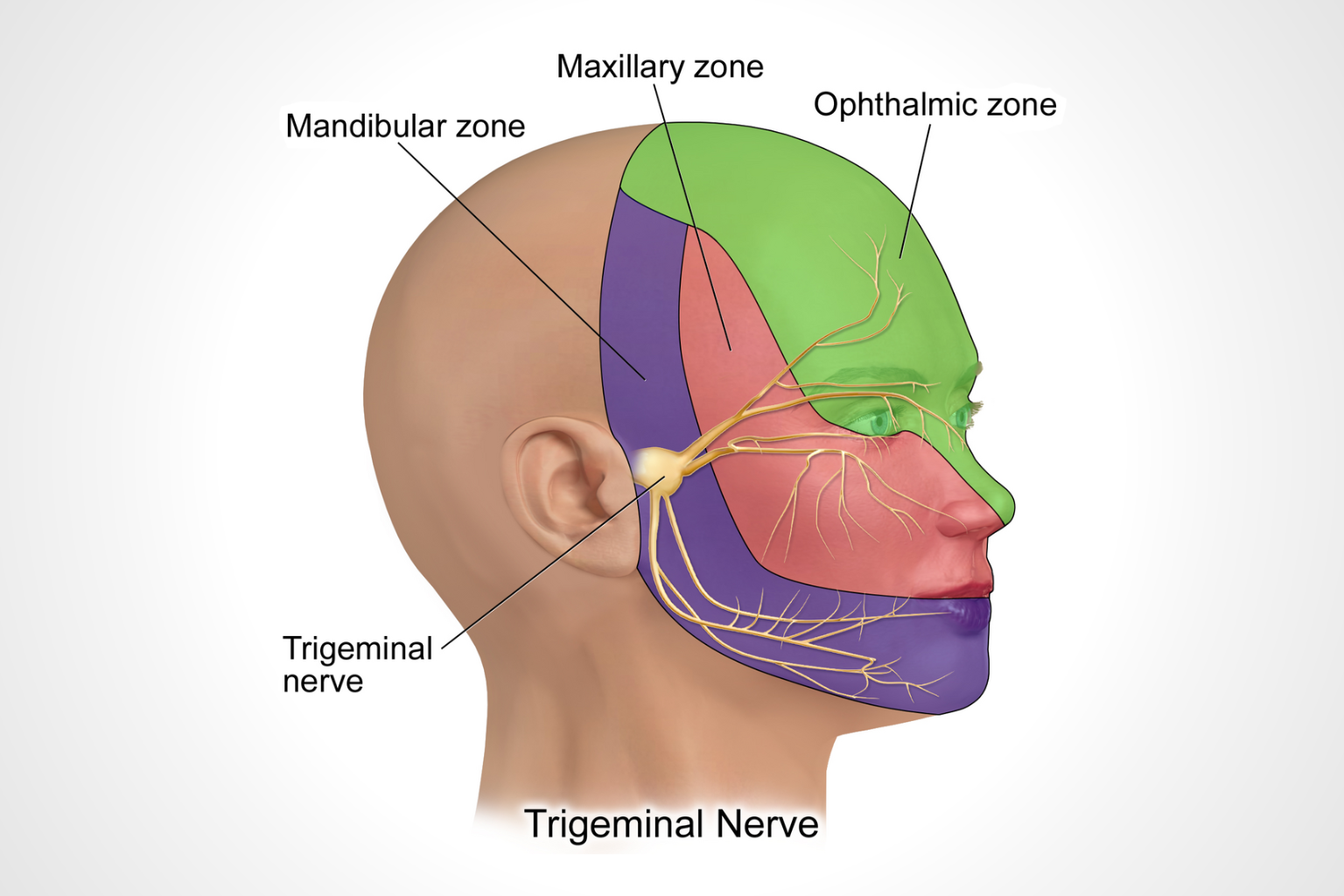
“Debbie,” a 52-year-old woman from the New York City metropolitan area, presented for consultation due to persistent bilateral burning pain following bilateral TMJ total joint replacement.
Two years earlier, she developed progressive jaw pain and limited opening secondary to severe degenerative joint disease. Conservative therapies, including oral appliance therapy, anti-inflammatory medications, and physical therapy, were unsuccessful, and she ultimately underwent bilateral total joint replacement.
Although mandibular function improved significantly postoperatively, she developed constant burning pain, described as “like my skin is sunburnt,” involving the temples and mandibular border.
Follow-up evaluations confirmed stable prostheses without mechanical complication. However, light palpation revealed hypoesthesia and allodynia, findings strongly supportive of post-surgical neuropathic facial pain. She had previously trialed NSAIDs, benzodiazepines, opioids, and anticonvulsants, all either ineffective or poorly tolerated.
When traditional neuropathic medications are ineffective or poorly tolerated, clinicians must reconsider the underlying pain mechanism and adjust treatment strategy accordingly.
Introducing Low-Dose Naltrexone (LDN) for Neuropathic Facial Pain

Naltrexone is an opioid blocker with a long history of use in the treatment of substance use disorders, typically dosed at 50 to 100mg daily. Low-Dose Naltrexone (LDN) refers to naltrexone prescribed at substantially lower doses, typically 1.5 to 6mg daily.
(Throughout this article, LDN refers exclusively to low-dose naltrexone.)
Why Low-Dose Naltrexone Can Be Effective for Neuropathic Facial Pain
LDN appears to act through two primary mechanisms.
Endogenous Opioid Upregulation
Endogenous opioids, or “endorphins,” serve as the body’s natural pain modulators. At low doses, naltrexone temporarily blocks opioid receptors for several hours. In response, the body increases endorphin production. When receptor blockade resolves, elevated endorphin levels bind to reopened receptors. In effect, LDN “tricks the body” into producing more of its own natural analgesics.
Microglial Modulation and Neuroinflammation Reduction
Microglia are immune cells within the central nervous system that, when chronically activated, release pro-inflammatory mediators contributing to central sensitization and persistent neuropathic pain. LDN appears to reduce microglial activation, thereby decreasing neuroinflammatory signaling and calming hypersensitive pain pathways.
Dosing and Prescribing Considerations
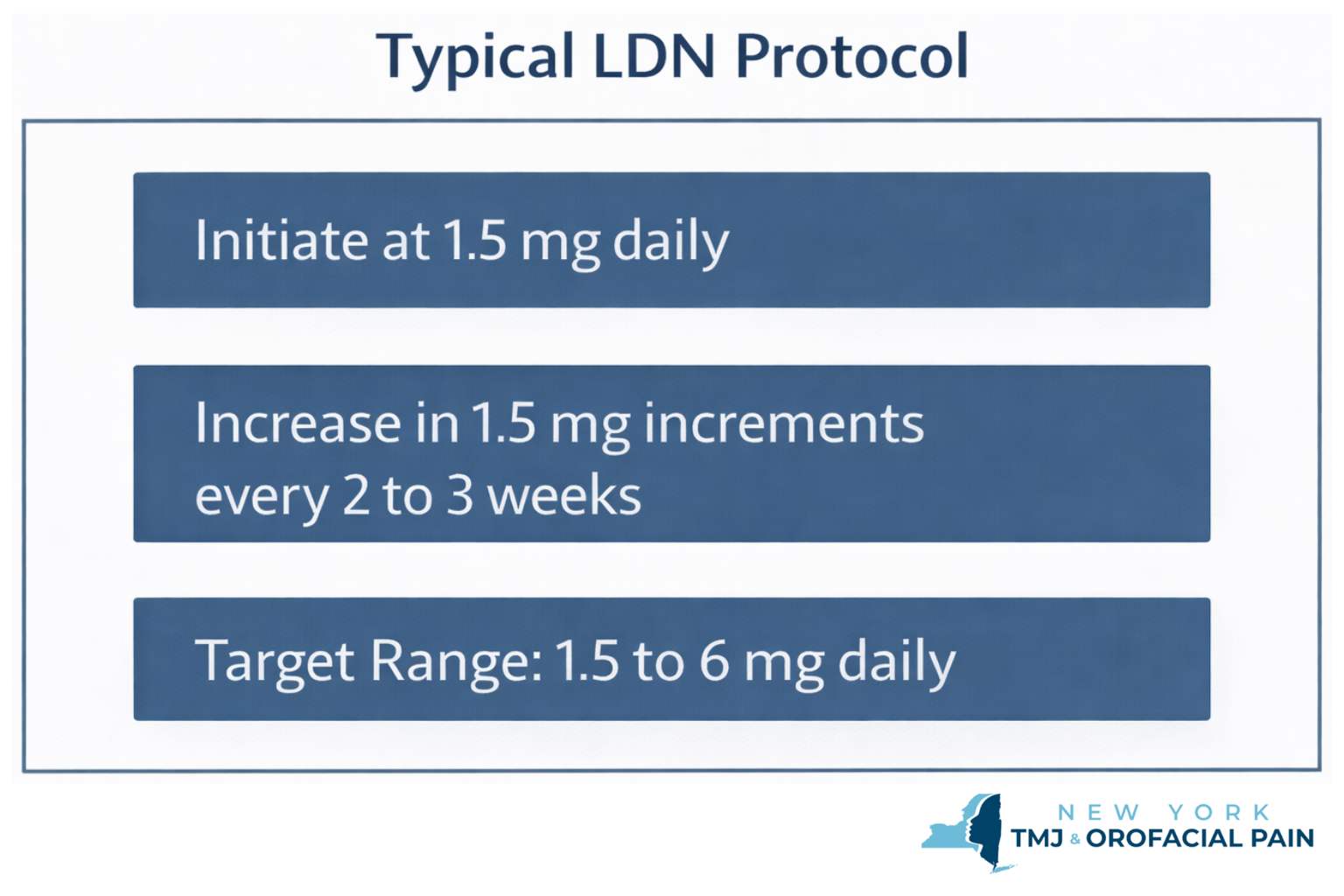
LDN must be obtained through a compounding pharmacy. Our typical titration protocol is outlined above.
Treatment is initiated at 1.5 mg daily, with gradual increases in 1.5 mg increments every 2 to 3 weeks, based on symptom response and tolerability.
Most patients respond within a range of 1.5 to 6 mg daily. Importantly, LDN demonstrates a therapeutic “sweet spot,” and both insufficient and excessive dosing may reduce clinical benefit. Individualized titration is essential.
Clinical Outcome
Debbie initiated LDN at 1.5 mg nightly. After minimal change, she increased to 3 mg. Within days, her burning pain decreased substantially. At 4.5 mg, symptoms intensified. Upon returning to 3 mg, improvement resumed.
At two-month follow-up, she reported she could still “feel her face,” but the sensation was no longer unpleasant or painful. She experienced no adverse effects.
Clinical Implications
Low-Dose Naltrexone for facial pain represents a low-risk, mechanism-based option for patients with:
- Persistent post-surgical TMJ pain
- Neuropathic facial pain
- Persistent idiopathic facial pain
- Persistent muscle pain
- Chronic headache disorders
- Burning mouth syndrome
For clinicians managing patients whose structural pathology has been corrected, but whose pain persists, LDN offers a targeted neuroinflammatory approach consistent with current understanding of centrally mediated pain.
Careful patient selection and dose titration remain essential.
If You Practice in the NYC Metro Area:
At New York TMJ & Orofacial Pain, we provide specialty-level evaluation and management of complex temporomandibular and orofacial pain disorders throughout the New York City metropolitan area, including Manhattan, White Plains, Long Island, and Springfield, New Jersey.
We are available for consultation and collaborative care with clinicians throughout NYC and the surrounding region.
The Author
Dr. John Dinan is a board-certified Orofacial Pain specialist dedicated to the treatment of TMJ/TMD disorders and related conditions. He practices in our Manhattan and Springfield, NJ offices.
Learn About Our Practice
Learn About Our Treatments
Read: Trigeminal Neuralgia and the Experience of Tooth Pain
Related Research: https://pubmed.ncbi.nlm.nih.gov/40271304/
