A mind-body disorder? Only some of the time
Temporomandibular disorders (TMD) do not all share the same origin. While some cases are influenced by mind-body mechanisms, others result from physical trauma or underlying medical conditions. Identifying the primary pathway is essential to selecting the correct treatment approach and preventing chronic dysfunction.
Introduction – the clinical challenge
When I look back retrospectively at the TMD problems I have evaluated over 43 years, many have been straightforward in their origin, identification, and management. Others, however, have posed challenges that stem from origins that are difficult to address and even more difficult to explain to patients who understandably want clear answers.
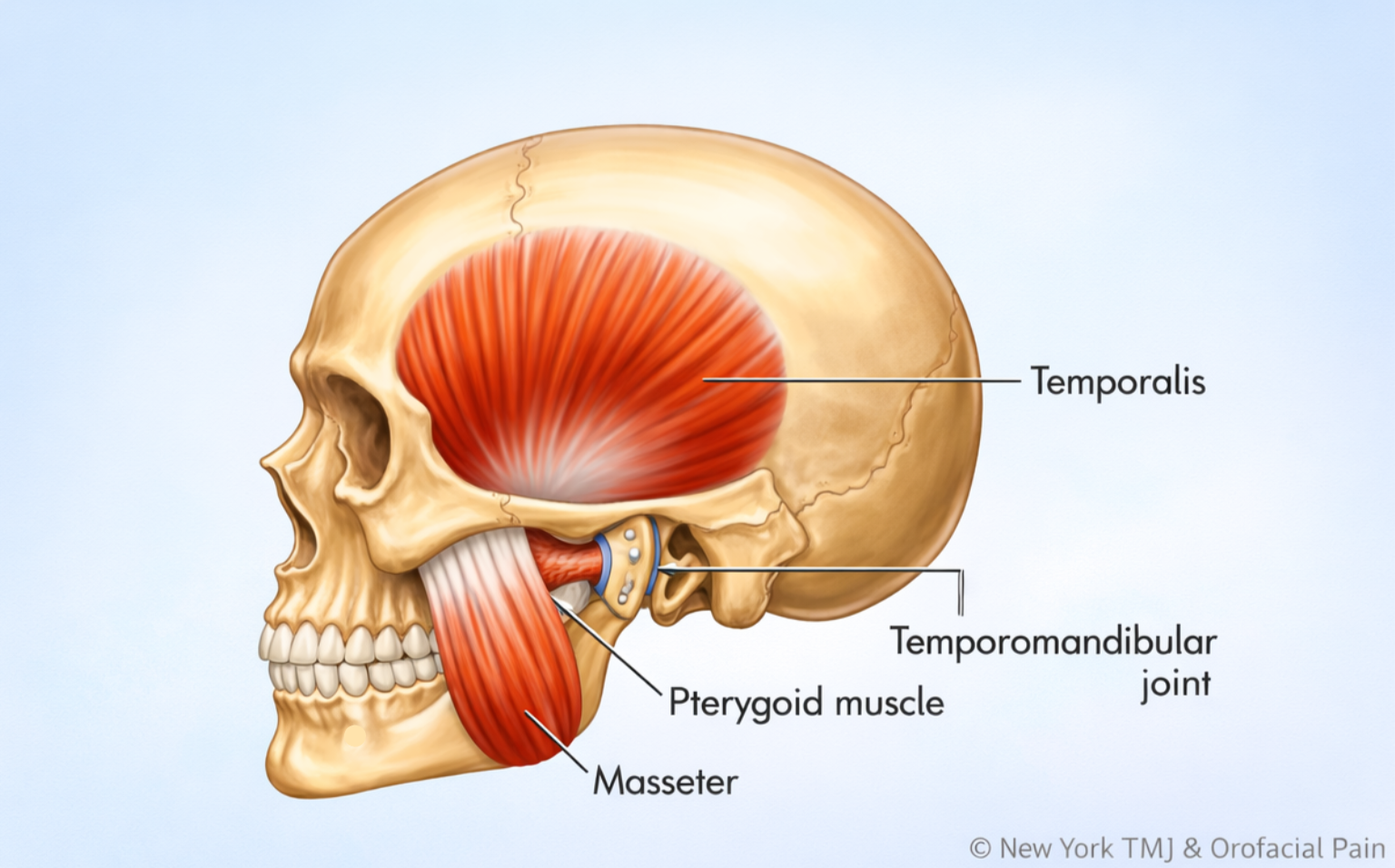
Temporomandibular problems are, in essence, orthopedic problems that result in pain and functional limitations. Patients’ symptoms and examination findings therefore tend to be predictable. This predictability has led to a group of treatment options that, when accurately chosen, reliably stop new tissue injury and support healing.
The most critical part of the initial doctor-patient relationship is figuring out the why. Understanding the origin of a patient’s problem is central to designing the appropriate management approach.
The mind-body connection has been cited as a potential cause of tissue injury, and I have written extensively about this relationship. However, it should not be assumed that emotional or psychological factors are the cause of every TMD problem.
The available literature emphasizes that TMD problems are multifactorial in origin, but this newsletter focuses on what I see as the three most common pathways driving the TMD problems we encounter in our offices:
- Mind-body disorders
- Traumatic origins
- Underlying medical conditions
Pathway one – mind-body disorders
When emotions drive physiology
Defining mind-body disorders
A mind-body disorder exists when physical symptoms and measurable dysfunction emerge and persist as a result of psychological and emotional factors that directly or indirectly trigger real physiological changes in the body.
Pain is described, and physical dysfunction is observed, such as limited jaw motion, for example, which may be noted during examination. Yet there is no single identifiable traumatic event or disease process to point to. Instead, the tissue changes responsible for these symptoms are driven by nervous system dysregulation, a state in which the autonomic nervous system (ANS), which controls automatic bodily functions, loses its normal balance and flexibility in responding to stress and returning to calm.
The mind-body cascade
From a theoretical perspective, if a mind-body disorder exists, the following sequence is possible.

Psychological triggers
Persistent emotional stress, early life trauma, PTSD, chronic anxiety, repressed anger, fear, or perceived threats, amongst other triggers, can activate the limbic system, our emotional processing center. This leads to increased sympathetic tone (fight-or-flight state), decreased parasympathetic tone (rest-and-digest state), and the release of cortisol and catecholamines.
Physiological changes
Over time, increased sympathetic tone leads to sustained muscle contraction, vasoconstriction, and reduced tissue oxygenation. This is followed by ATP depletion (source of cellular energy) and increased lactic acid accumulation.
Tissue impact
This cascade can create microtrauma to ligaments, capsules, muscles, and tendons, leading to consequential pain and dysfunction. The resulting problems may involve both muscle and joint tissues, including soreness, referred pain, tendinitis, joint sprains, disc interference, and arthritis.
The resulting symptoms can be indistinguishable from those caused by actual traumatic events or underlying medical disorders.
Clinical presentation and profile
This cascade explains a percentage of the patients we see every year. Their histories are often free of specific or identifiable traumatic events or underlying medical conditions. Many describe years of “TMJ” problems with waxing and waning symptoms that have recently intensified.
Most are between the ages of 17 and 55, and approximately 70 percent are female. Many report anxiety, depression, and ongoing stress-related challenges. While countless others share this profile without experiencing TMD, this presentation is strikingly common in clinical practice.
Chronic microtrauma as a contributing factor
As a result of the common psychological triggers seen in this population, chronic repetitive microtrauma may also occur. Daytime jaw overuse behaviors and fatiguing head and neck postures are frequently observed.
Daytime constant tooth contact, clenching, nail and cuticle biting, pen chewing, habitual jaw tensing, and work-related forward head posture can all place the jaw and neck muscles and temporomandibular joints at increased risk. In addition, aggressive sleep bruxism, driven by heightened sympathetic states, can affect the TM joints and jaw muscles night after night, potentially leading to injury.
For these patients, meaningful improvement often requires a team-based approach.
Pathway two – traumatic origins
When physical injury initiates the problem
The second pathway to TMD is often the most straightforward to identify: direct physical trauma to the jaw structures. Unlike mind-body TMD, where symptoms arise without a clear precipitating event, trauma-induced TMD frequently has an identifiable moment of injury.
The events may vary, but they share a common thread. Forces applied to the temporomandibular joints and surrounding muscles, tendons, and ligaments exceed their capacity to absorb impact, and tissue damage occurs.
Acute trauma
Sports-related impacts, motor vehicle accidents, and accidental blows to the chin or jaw can cause immediate structural damage, including sprained ligaments and disc displacements, along with profound inflammation.
Trauma does not need to be dramatic to cause problems. Injuries during medical and dental procedures are common. Prolonged mouth opening during general anesthesia intubation or extended jaw opening during dental procedures can strain tendons, sprain ligaments, and initiate inflammation in joint tissues. Intimacy can also be responsible for muscle and joint compromises.
Dietary choices may also contribute. Biting hard foods such as a tough bagel, an overly crusty baguette, or a biscotti cookie can create an acute joint sprain as well. Opening too wide to bite into an apple or a large sandwich can also unexpectedly lead to injury. Patients often recall the moment clearly: “I bit down on something hard and felt a pop.”
Clinical distinction
In trauma-induced TMD, the initial injury triggers inflammation, protective muscle splinting, and altered joint mechanics. If healing remains incomplete, the acute injury may progress to chronic dysfunction.
The distinguishing feature is a clear historical event, often accompanied by unilateral symptoms corresponding to the side of injury.
Pathway three – underlying medical conditions
The predisposed patient
The third pathway involves patients whose TMD arises not from stress or trauma but from underlying medical conditions that predispose the temporomandibular system to injury and dysfunction. These individuals have genetic, systemic, or metabolic vulnerabilities that make their joints and connective tissues less resilient.
Connective tissue disorders
Hypermobility disorders, particularly Ehlers-Danlos syndrome, are significant predisposing factors. These patients have abnormally elastic and fragile collagen, resulting in joint laxity, ligament instability, and poor tissue repair. Even routine activities such as yawning or eating may destabilize the temporomandibular joints. What is benign for most people, such as chewing gum or eating a tough piece of meat, may be injurious for hypermobile patients.
Inflammatory arthritides
Conditions such as rheumatoid arthritis, psoriatic arthritis, and other autoimmune disorders may involve the temporomandibular joint, leading to synovial inflammation, cartilage degradation, and bone erosion. Degenerative conditions such as osteoarthritis also predispose the joint to pain and dysfunction.
Neurological and hormonal factors
Oromandibular dystonia, a neurological movement disorder characterized by involuntary jaw contractions, subjects the joint to abnormal forces. Hormonal conditions, particularly those involving estrogen levels, appear to influence TMD susceptibility. This helps explain why TMD affects women disproportionately and why symptoms may fluctuate with menstrual cycles or menopause.
Predisposition and behavior
Predisposition does not mean inevitability. Not all hypermobile or arthritic patients develop TMD. These conditions create vulnerability rather than certainty. Additional factors such as muscle tension, jaw overuse behaviors, postural strain, or minor trauma often contribute to symptom development.
A patient with Ehlers-Danlos syndrome who develops TMD presents a different clinical picture than a patient with trauma-based or stress-related origins. Treatment must address both the underlying condition and the daily activities and behaviors that exacerbate it. The goal shifts from resolution to long-term management, helping patients work within their body’s limitations while maintaining quality of life.
Integrating the pathways – one clinical goal: find the why
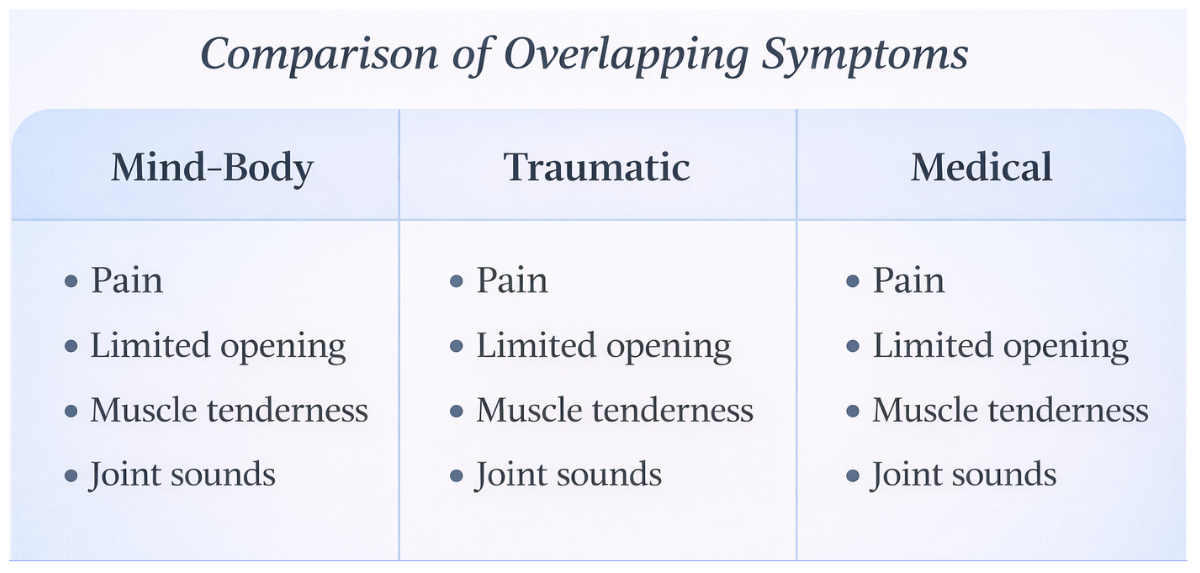
The clinical presentations of these three TMD origins, mind-body, traumatic, and medically predisposed, can appear remarkably similar. All may present with pain, limited opening, muscle tenderness, joint sounds, and functional limitations.
The clinician’s task is to carefully distinguish among them through detailed history-taking, examination, and appropriate testing. The why determines the how of treatment.
Each pathway is real. Each requires its own therapeutic approach. Recognizing which pathway applies to each patient remains the cornerstone of effective TMD management.
Related clinical topics:
- Sarno and My Approach to TMJ
- TMD Problems: Why So Many Women?
- Advances in Temporomandibular Disorders: Insights for Dental Professionals
- Additional Insights From The NYTMJ Professional Newsletter
Frequently asked questions about pathways to TMD
-
What are the most common causes of TMD?
The most common causes of TMD fall into three categories: mind-body disorders, physical trauma, and underlying medical conditions.
-
Is TMD always a mind-body disorder?
No. While mind-body mechanisms play a role in some cases, many patients develop TMD due to physical injury or medical predisposition.
-
How can clinicians tell if TMD is mind-body or trauma-related?
The key difference is patient history. Trauma-related TMD usually follows a clear physical event, while mind-body TMD often develops without a specific injury.
-
How does nervous system dysregulation cause jaw pain?
Nervous system dysregulation can cause prolonged muscle tension and reduced blood flow, leading to pain and tissue injury over time.
-
Can stress cause real tissue injury in TMD?
Yes. Stress can lead to real physiologic changes that result in actual tissue injury, not just pain perception.
-
How does trauma lead to chronic TMD?
Trauma can damage joint or muscle structures, and incomplete healing can allow acute injury to progress to chronic dysfunction.
-
Why are Ehlers-Danlos patients more prone to TMD?
Fragile connective tissue and joint instability increase susceptibility to repetitive injury.
-
How do hormones affect TMD?
Estrogen fluctuations influence joint tissues and pain sensitivity, contributing to higher prevalence in women.
-
Why do different TMD causes look the same clinically?
Different causes often lead to the same final symptoms, making etiology essential for diagnosis.
-
Why is identifying the why of TMD important?
Because treatment depends on the cause, and symptoms alone do not guide effective care.
