
This content was originally published on 2/9/2022 and reviewed on 6/19/2026.
When patients come to my office with the complaint of persistent (and often acute) pain in their face or jaw, they often fear they have a problem called trigeminal neuralgia.
Before discussing this specific type of facial pain, a brief discussion about the trigeminal nerve and its role in virtually all facial pain problems is essential.
The trigeminal nerve is but one of 12 cranial nerves that can transmit two types of information to the brain.
- Sensory Information: Includes details about smells, sights, tastes, touch, sounds, and PAIN to the brain.
- Motor Information: Initiates movement or activation of muscles and glands.
The Three Branches of the Trigeminal Nerve
The trigeminal nerve has three different divisions, each with a slightly different function:
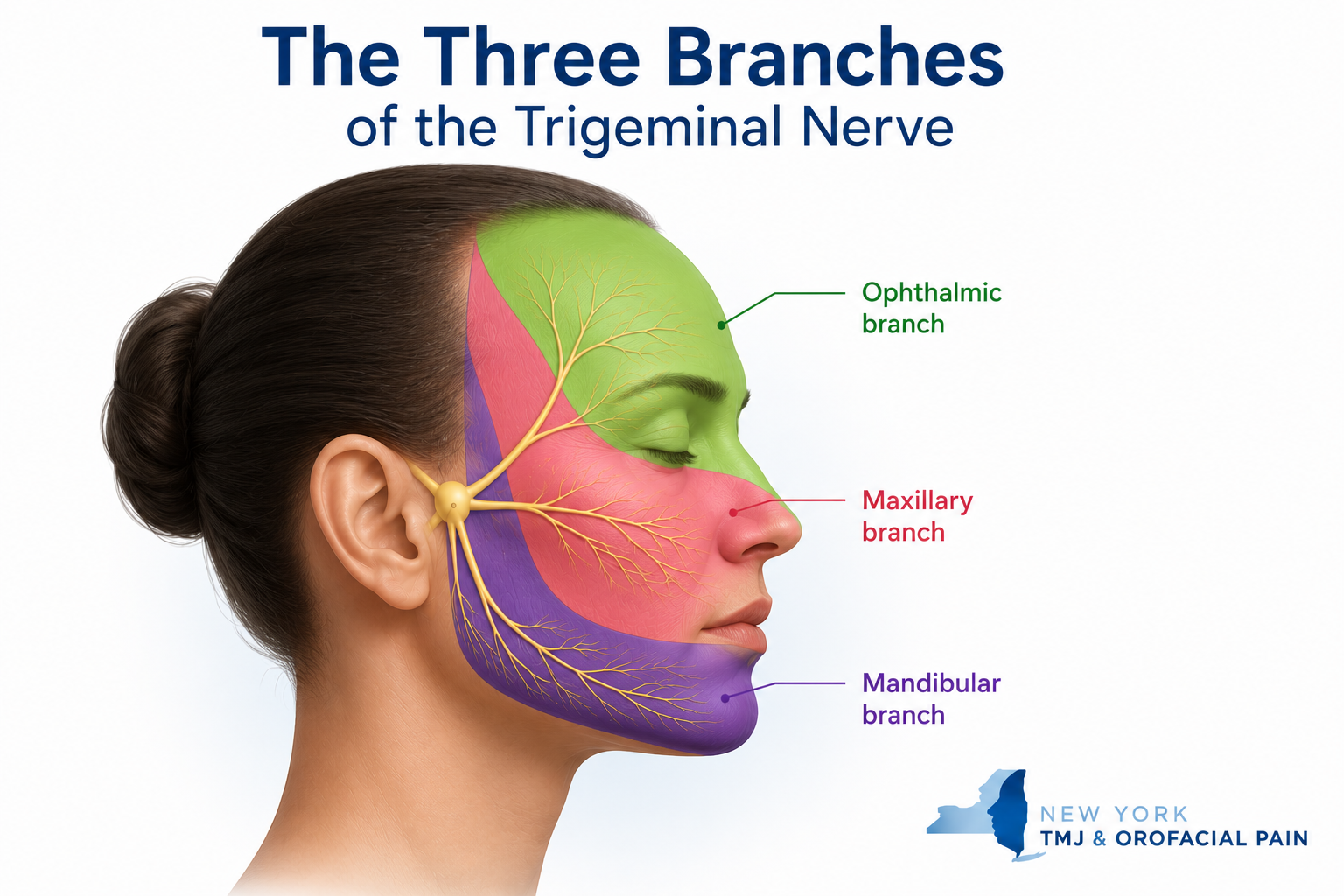
1. The Ophthalmic Division
The ophthalmic division transmits sensory Information to the brain from:
- The scalp
- The forehead
- The upper sinuses
- The upper eyelid and associated mucous membranes
- The cornea of the eye
- The bridge of the nose
2. The Maxillary Division
Like the ophthalmic division, the maxillary division of your trigeminal nerve has only a sensory component. It transmits sensory Information to the brain from:
- The lower eyelid and associated mucous membranes
- The middle part of the sinuses
- The nasal cavity and middle part of the nose
- The cheeks
- The upper lip
- The teeth of the upper jaw and the surrounding gum tissue and supporting bone
- The roof of the mouth
3. The Mandibular Division
The mandibular division is the only part of the trigeminal nerve that has both sensory and motor functions. It communicates sensory Information to the brain from:
- The outer part of the ear
- The lower part of the mouth and the associated mucous membranes
- The front and middle parts of the tongue
- The teeth of the lower jaw and the associated gum tissue and supporting bone
- The lower lip
- The chin
- The temporomandibular joint and jaw muscles
The mandibular division also stimulates movement of the muscles in the jaw and some of the muscles within the inner ear.
What Is Trigeminal Nerve Pain?
As a result of the trigeminal nerve’s sensory function and broad distribution in the intraoral tissues, facial and jaw structures, the majority of all orofacial pain is due to excitation, irritation, and or injury to the trigeminal nerve.
Common toothaches, wisdom tooth pain, dental infections, sinus pains, jaw muscle pain, and temporomandibular joint pain all involve the trigeminal nerve. Therefore, trigeminal nerve pain can result from an overworked and fatigued jaw muscle, an inflamed jaw joint, a cracked or decayed tooth, or a simple gum infection.
Therefore, most of the suffering due to trigeminal nerve pain occurs as a result of problems that can be readily diagnosed and treated effectively by trained practitioners. Most importantly, these problems are common, familiar, and helpable when evaluated and treated by trained practitioners.
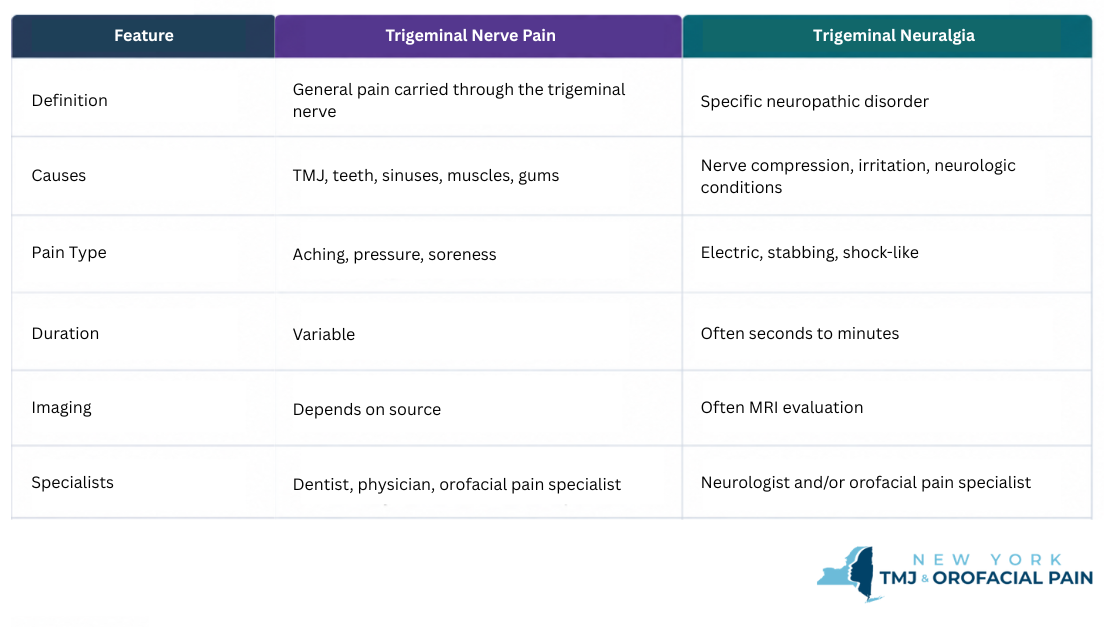
What is the difference between trigeminal nerve pain and trigeminal neuralgia?
Trigeminal nerve pain is a broad term describing pain signals carried by the trigeminal nerve from the teeth, jaw muscles, TMJ, gums, sinuses, or facial tissues. Trigeminal neuralgia is a specific neuropathic pain disorder that usually causes sudden, severe, electric-shock-like facial pain.
Because both conditions involve the trigeminal nerve, trigeminal neuralgia can sometimes feel like tooth pain, jaw pain, or a TMJ problem. A careful history, examination, and sometimes imaging are needed to determine the true source of pain.
For patients who have undergone multiple dental, medical, or TMJ evaluations without a clear diagnosis, an orofacial pain evaluation can help identify whether symptoms are more consistent with trigeminal neuralgia, TMJ-related pain, dental pain, or another facial pain condition.
What Is Trigeminal Neuralgia?
Trigeminal neuralgia (TN) is a distressingly painful, sometimes debilitating, and often chronic neuropathic pain condition. Trigeminal neuralgia typically affects the middle or the lower part of the face on one side. As it is classified as a type of neuropathic pain, it is mostly caused by damage or disease to the nervous system’s sensory component.
Trigeminal neuralgia becomes more common as people reach their 60s and 70s and can be triggered by a variety of serious medical conditions such as tumors, stroke, multiple sclerosis, and other disorders that cause the insulation of trigeminal nerve fibers to become compromised. According to the National Institute of Neurological Disorders and Stroke, the incidence of new cases is approximately 12 per 100,000 people per year; the disorder is more common in women than in men.
The pain of trigeminal neuralgia can be felt in the face, teeth, gums, lips, and mouth region and tends to be sporadic, electrical or shock-like, and is often combined with a burning sensation. Patients frequently describe spark like electrical sensations during an attack.
Approximately 60% of all patients often diagnosed with trigeminal neuralgia start seeking care from a dentist because they are experiencing bad toothache pain. Yet, evaluations and x-rays taken in the dental office usually do not reveal the real problem. Despite a lack of findings, treatment such as root canals is often initiated treatment such as root canals are often started as a way to relieve a patient’s suffering. Unfortunately, these efforts fail to solve the problem.
To learn more about trigeminal neuralgia, visit Johns Hopkins Medicaine – Trigeminal Neuralgia.
How Trigeminal Neuralgia Is Diagnosed
The pain of TN has some unique features. The pain may be experienced in the midst of an otherwise pain-free day appearing without provocation, or it can be triggered by speaking, drinking, eating, brushing the teeth, or causal contact of the face around the lips and nose.
Unlike most other facial pain problems, trigeminal neuralgia pain can be manageable or miserable all within several minutes of a day. People with trigeminal neuralgia often report being pain-free and then incapacitated for seconds or minutes until the pain vanishes or subsides to a low level. Trigeminal neuralgia attacks can become more frequent and intense over time.
Why Trigeminal Neuralgia Can Feel Like a TMJ Problem
Patients with trigeminal neuralgia often describe severe limitation of jaw motion during an attack of TN due to spasm of the jaw muscles, which are directly under the influence of the trigeminal nerve. For this reason, TN has also been called tic douloureux, with the ‘tic’ describing the severe facial muscle spasm. Due to the restricted jaw motion described by patients, this problem can be misdiagnosed as TMJ.
As mentioned, the diagnosis of trigeminal neuralgia is most commonly made based on the unique character of the symptoms the patient describes. The examination of the face and the painful areas is often unremarkable unless there are distinct trigger zones that, when touched, fires the pain.
Brain imaging MRIs or MRAs may be ordered in order to detect whether there is an underlying medical condition such as MS, a tumor, or blood vessel compression of the nerve causing the TN pain.
Finally, trauma to the face, jaw, or teeth can injure the trigeminal nerve and lead to what is called traumatic TN.
Common Treatment Options for Trigeminal Neuralgia
Once a tentative diagnosis has been made, medications are usually the first-line treatments. Multiple medications may be used together and changed over time if effectiveness is lost. These medications are designed to reduce the nerve sparking and excitation, but unfortunately do not cure trigeminal neuralgia.
Other treatments may be beneficial as well, including nerve blocks and, at times, BOTOX® injections. Topical medications, both inside the mouth and on the face, have also shown some promise in controlling daily symptoms.
When these treatment efforts fall short despite collaboration with multiple experts in the field, neurosurgery is the next step to be explored.
Other Types of Trigeminal Neuropathic Pain
There is an “atypical” form of TN called TN2. Instead of short episodes of disabling pain, patients with TN2 experience continuous pain with burning and aching features. Although the pain of TN2 is less intense than TN, its constant presence is often thought to be more disruptive to a patient’s life as there is no downtime.
Continuous neuropathic pain problems also require medications to ease suffering. However, because continuous nerve pain can lead to muscle tension and splinting, TN2 symptoms can be confused with a TMJ problem.
In summary, pain within the trigeminal system is a primary reason that patients seek care in my practice. Fortunately, once a diagnosis has been made, many of these problems are common, familiar, and helpable.
If you or someone you know is experiencing persistent or acute pain in the face or jaw, we invite you to set up a consultation with one of our Orofacial Pain specialists in the NYC metropolitan area. Our office locations and contact information are below.
Not Sure If Your Pain Is TMJ, Tooth Pain, or Trigeminal Neuralgia?
Facial pain can be difficult to diagnose because the trigeminal nerve carries pain signals from many facial structures.
If your pain has not been clearly diagnosed, an orofacial pain evaluation can help determine the most likely source.
New York TMJ & Orofacial Pain evaluates patients with facial pain, jaw pain, tooth-like pain, TMJ symptoms, and nerve-related pain at office locations in Manhattan, Long Island, Westchester, and Northern New Jersey.
Contact us today to schedule a comprehensive evaluation. →About the Author
Donald R. Tanenbaum, DDS, MPH, is Co-Founder of New York TMJ & Orofacial Pain and a board-certified specialist in Orofacial Pain. Together with his colleagues, he helps evaluate and manage patients with temporomandibular disorders (TMD), complex facial pain, neuropathic pain conditions, headaches, and sleep-related disorders. New York TMJ & Orofacial Pain is a referral resource for medical and dental professionals seeking specialized care for patients with challenging orofacial pain and jaw disorders. The practice has office locations in Manhattan, Long Island, Westchester, and Northern New Jersey.
Frequently Asked Questions Trigeminal Nerve Pain vs. Trigeminal Neuralgia
Is trigeminal nerve pain the same as trigeminal neuralgia?
No. Trigeminal nerve pain is a broad description of pain carried by the trigeminal nerve. Trigeminal neuralgia is a specific neuropathic pain disorder.
Can trigeminal neuralgia feel like TMJ?
Yes. Many patients initially believe they have TMJ pain because trigeminal neuralgia can affect the jaw area.
Can trigeminal neuralgia feel like a toothache?
Yes. Trigeminal neuralgia frequently mimics dental pain and may lead patients to seek dental treatment before receiving an accurate diagnosis.
What does trigeminal neuralgia pain feel like?
Patients often describe sudden electric-shock-like, stabbing, or burning facial pain.
Who should I see for facial pain that might be trigeminal neuralgia?
A neurologist and/or an orofacial pain specialist may be involved depending on the symptoms and diagnosis.
Can TMJ problems irritate the trigeminal nerve?
TMJ disorders can generate pain signals carried by the trigeminal nerve, but this does not necessarily mean a patient has trigeminal neuralgia.
When should someone in the NYC area see an orofacial pain specialist?
Patients should seek evaluation when facial pain, jaw pain, tooth-like pain, or nerve pain persists despite prior dental or medical treatment, or when the diagnosis remains unclear.







9 comments on “Trigeminal Nerve Pain vs. Trigeminal Neuralgia: What’s the Difference?”
Reading on TN tonight and came across your website, I had mri. ruled out any tumor, compression or ms .
Your website sounds promising to get relief i seen yall are in NY im in Ala , do u have a office closer to Ala
Hi Christa,
Sorry to hear about your troubles. You can find orofacial pain specialists in your area here.
Best of luck,
Dr. Tanenbaum
I am in Australia and read your information as l have a neuralgia like pain in the left side of my face, around my ear and jaw. Been there for about 8 weeks, or more. cannot sleep on that side. No dental or ear issues aside from getting water in ear in about March but l got Dr review then. Ears are NAD. Got ENT referral yesterday. Might be TN2? I am quite worried. Thanks for the Info.
Hi Judith,
So sorry to hear of your troubles. It sounds like you are on the right track. If nothing helps after the ENT see if you can find an Orofacial Pain Specialist in your area.
Best of luck,
Dr. Tanenbaum
I have been diagnosed with TN. Tegretol used to work. Now the pain is daily and feels like it’s in the jaw joint making it very difficult to speak more then a sentence without excruciating pain. Im not even able to kiss my great grand baby without severe pain. Its extremely depressing. Are there groups for support?
Lisa, I’m sorry to hear of your troubles. If you are in the U.S., please check out the Facial Pain Association. They have tons of resources including support groups.
The best of luck to you.
Dr. Tanenbaum
I read your website. I have been experiencing jaw pain and hyper ear sensitivity for twelve weeks. I also had a severe tension headache that went away but I continue to feel “off” simply quite not there. Almsot like if I am on a boat. I went from a super healthy person to waking up with a massive headache and jaw/ear pain. I have had so many doctors not know what’s wrong with me… until recently I was diagnosed with TN and put on Gabapentin. I don’t do well with meds. But could it be TMJ? I also have a c5c6 8.7mm stenosis but only the chiropractor thinks it’s related. I am miserable . I live in the capital of the medical world… Houston, and yet no doctor has been able to fully help me. I would travel anywhere. I am misrable.
Dear Amy,
I’m sorry to hear about your health troubles. I won’t be able to diagnose you without seeing you in person, but I’d suggest finding an orofacial pain specialist near Houston. Here’s the directory.
Best of luck! I hope you feel better soon.
Dr Tanenbaum